Downloaded 716 times
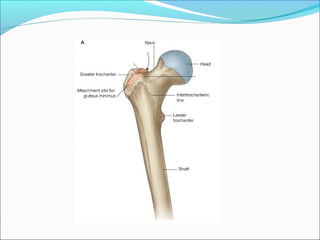
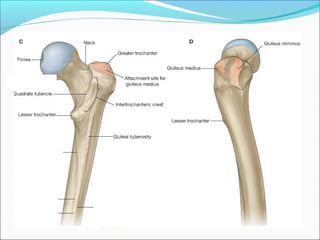
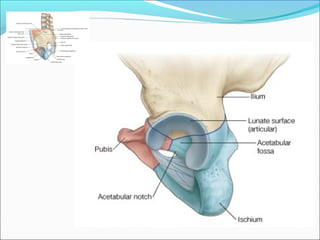
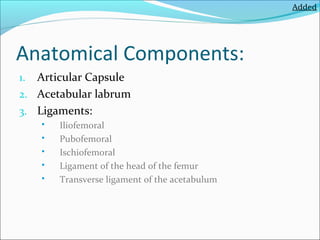
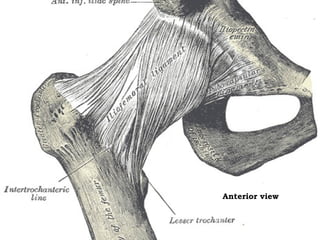
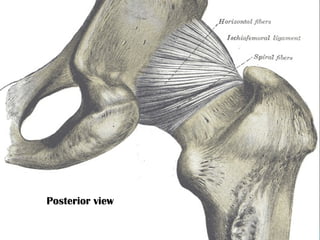
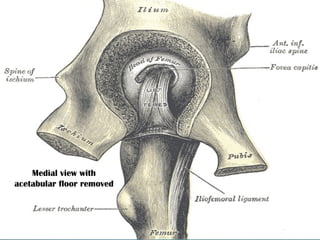
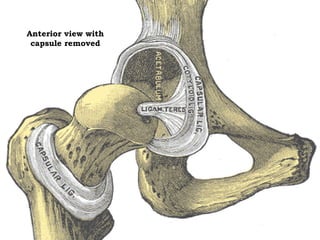
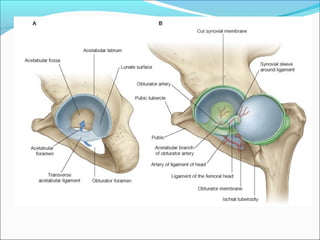
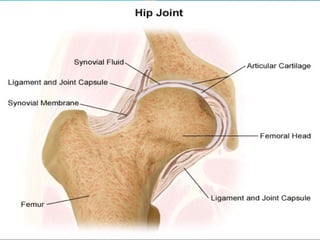
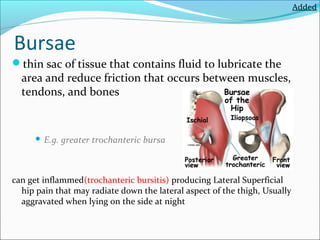
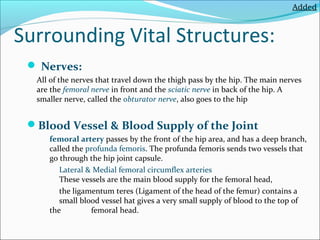
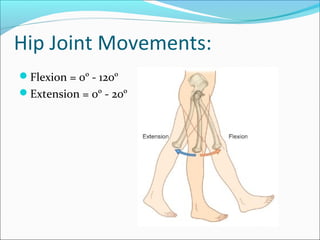
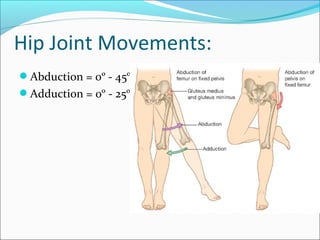
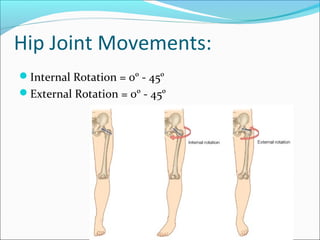
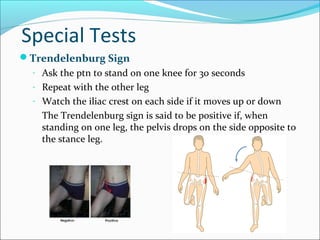
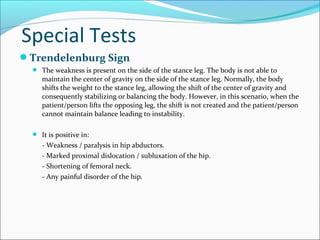

The hip joint is a ball and socket joint that connects the femur to the pelvis. It has an articular capsule and several ligaments that provide stability. Important anatomical structures near the hip joint include nerves, blood vessels, and bursae. The hip allows flexion, extension, abduction, adduction, internal and external rotation. Examination of the hip evaluates gait, range of motion, special tests like Trendelenburg sign, and imaging may be used.























































































