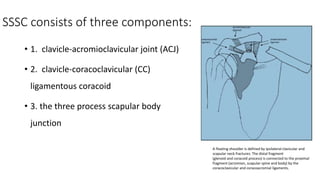
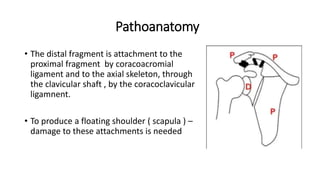
1) A floating shoulder injury involves concurrent fractures of the ipsilateral clavicle and scapular neck.
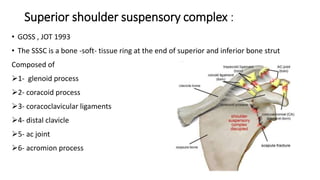
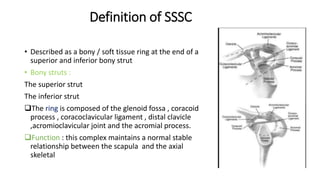
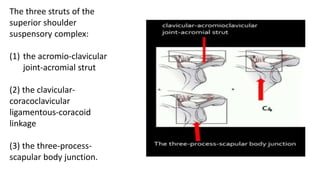
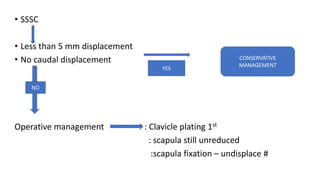
2) The superior shoulder suspensory complex (SSSC) is a bone and soft tissue structure that connects the scapula, clavicle, and coracoid process to maintain shoulder stability.
3) Floating shoulder injuries are often high-energy injuries associated with other fractures and injuries. Surgical treatment is usually indicated for significantly displaced or articular fractures to restore anatomy and function.