Downloaded 139 times
![ Early days – congenital deformity.
Smillie [1768] – Obstetric origin
Danyau [1851] – Autopsy – lesion
Duchenne [1861]- traction injury, OBPI
ERB [1875]- pointed lesion at upper trunk
Kennedy [1903]- early surgical repair
Narakas [1981]- microsurgical results.](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-2-320.jpg)
![ Incidence: 4/1000 in poor OBG care, 0.1-0.3
% in good centers.
1% of OBPP, injury is bilateral
More on one side. [exclusive in breach]](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-3-320.jpg)
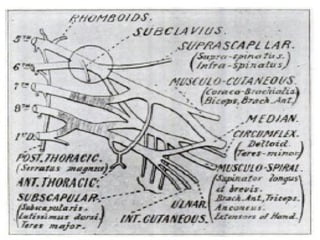
![ Formed by anterior primary rami of C5-T1.
Roots – between scalene muscles
Trunks – posterior triangle
Divisions- behind clavicle.
Cords in axilla.
Roots & trunk- supraclavicular part [OBPP]
Cords & branches – infraclavicular part](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-4-320.jpg)
![ Large birth weight
Breech presentation
Maternal diabetes
Multiparity
II stage of labour - > 60 min
Assisted delivery [forceps, vacuum ext]
previous child with OBPP
Intrauterine torticollis
Shoulder dystocia](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-7-320.jpg)
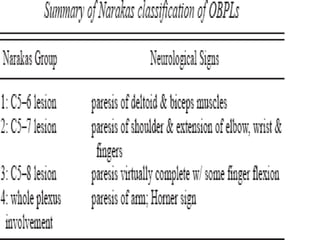
![ Lesions range from degree I[neuropraxia] – V
[neurotmesis or root avulsions].
Upper trunk –1st
affected, most vulnerable
part.
Upper trunk – mostly stretched
Lower trunks – mostly ruptured](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-8-320.jpg)
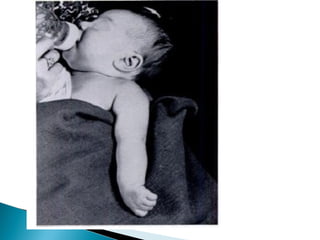
![ U.E is flail & dangling
Look for other extremities
U.R: arm held in IR,add, active abd not
possible, elbow extended forearm pronated,
thumb flexed.
Complete paralysis- vasomotor impairment,
pale & marble like color
Horner’s sign
Associated # [clavicle,humerus,]](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-9-320.jpg)
![ Nature of injury [rupture better]
Lower plexus paralysis,
global involvement,
persistence of pupillary signs of phrenic nerve
palsy
Ass. #.](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-19-320.jpg)

![ To predict poor outcomes if microsurgical
repair or grafting is not done.
scale consists of grading elbow flexion,
elbow extension, wrist extension, finger
extension, and thumb extension. [max -12]
score of < 3.5 predicted a poor long-term
outcome without microsurgery.](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-27-320.jpg)
![ Fracture of clavicle or humerus shaft or physeal
separation
septic arthritis / osteomyelitis
Congenital malformation of plexus
Postinfectious [varicella] plexopathy of muscles](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-28-320.jpg)
![ Sequelae depends on three factors which
are additive
1. Paralysis of muscle groups [ext.rot, elbow
flexors]
2. Contracture of healthy antagonist muscles
3. Impaired growth osseous deformities
Sequale – seen in spontaneous recovery in
gr III & IV lesion.](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-31-320.jpg)
![ Between shoulder abductors [S.S, I.S ,del] &
adductors [pect maj, ter.m] limitation of
shoulder elevation
Elbow flexors [biceps & brachialis] & elbow
extensors [triceps]
Elbow flexors & shoulder abductors trumpet
sign
Shou abd, elb flex,forearm flex](https://image.slidesharecdn.com/obpp-130423122747-phpapp01/85/Obstetric-brachial-plexus-Palsy-32-320.jpg)
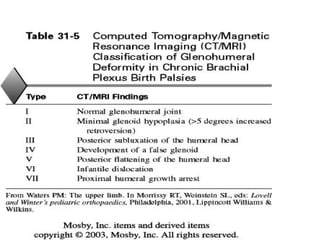
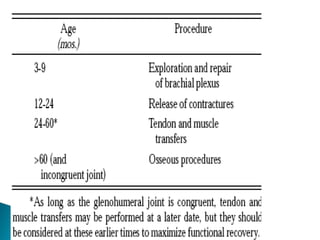

This document discusses obstetric brachial plexus palsy (OBPP), including its causes, presentation, evaluation, treatment, and long-term management. It notes that OBPP is caused by stretching or avulsion of the brachial plexus nerves during childbirth. Clinical assessment focuses on determining the specific roots involved and severity of injury. Management involves initial physiotherapy followed by surgical repair or reconstruction if needed to address nerve injuries or resulting musculoskeletal deformities. The goal is to restore function and prevent long-term complications through a multidisciplinary approach.








































![Osteosarcoma[2]](https://cdn.slidesharecdn.com/ss_thumbnails/osteosarcoma2-130423123803-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Odu%20 clinical%20science%20iii%20bpi%202011[1]](https://cdn.slidesharecdn.com/ss_thumbnails/odu20clinical20science20iii20bpi2020111-111213214145-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























