Downloaded 2,511 times
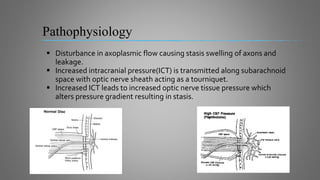
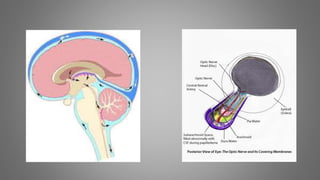
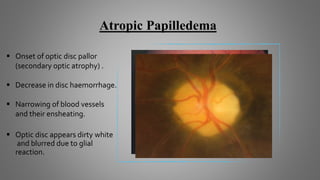
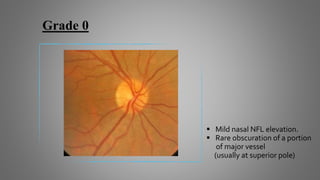
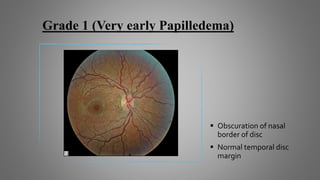
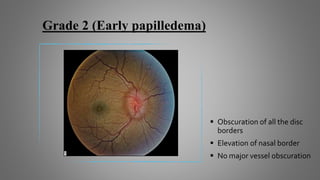
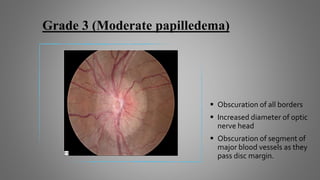
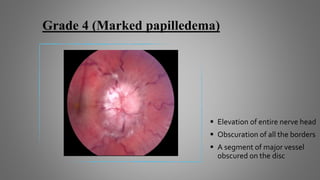
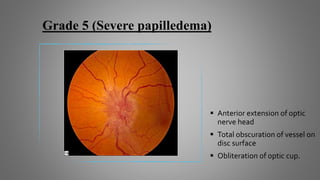
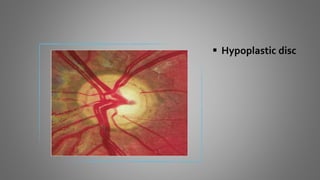


This document discusses papilledema, which is swelling of the optic disc due to increased intracranial pressure. It defines papilledema and outlines its causes, signs, symptoms, grading, histopathology, investigations, differential diagnosis, and treatment. The main points are that papilledema is caused by increased intracranial pressure, it can be graded on a scale from 0-5 based on severity, and treatment involves addressing the underlying cause of pressure increase as well as surgical decompression in severe cases to prevent vision loss.























































































