Downloaded 40 times

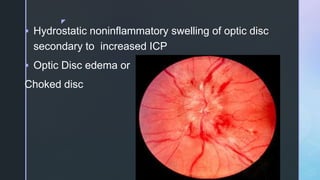




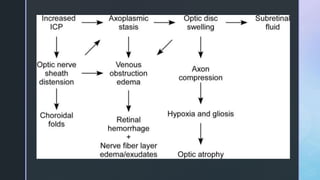
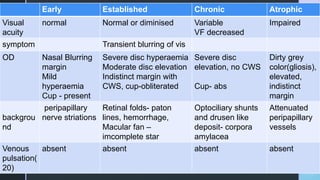
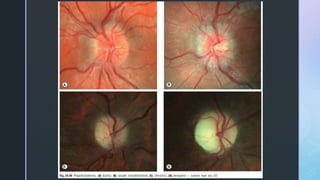

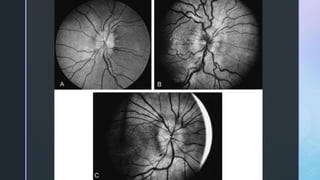

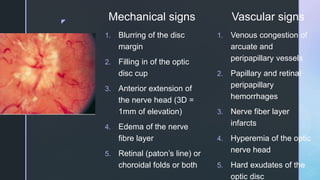
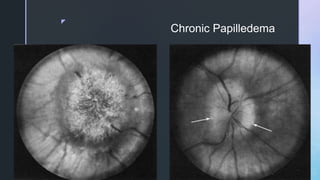
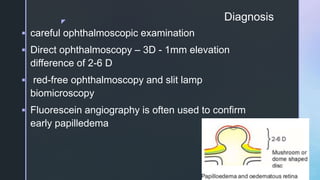
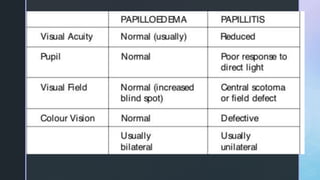

Papilledema is swelling of the optic disc caused by increased intracranial pressure. It is characterized by blurred disc margins and retinal nerve fiber layer edema. Increased CSF pressure is transmitted through the subarachnoid space and causes axoplasmic stasis in the optic nerve head. Papilledema is graded based on degree of disc elevation and obscuration from Frisen scale 0-5. Treatment involves addressing the underlying cause of increased ICP through medications, repeated lumbar punctures, or neurosurgery.












































![fundoscopy and papilledema ophthalmology [2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fundoscopyandpapilledema2-250809170746-59ac9d61-thumbnail.jpg?width=640&height=640&fit=bounds)































