

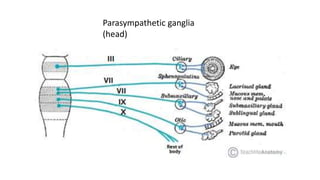

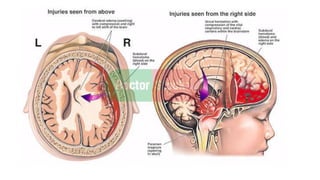

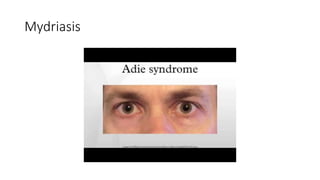
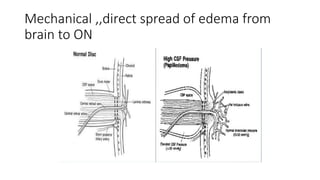
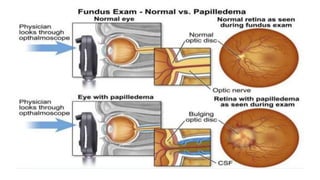
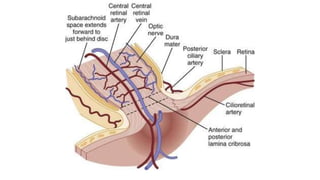
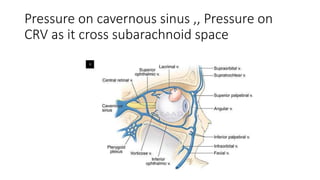
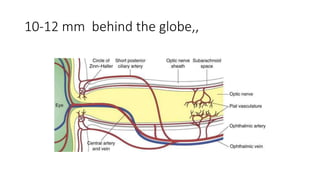
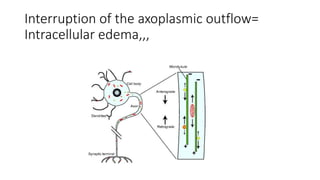
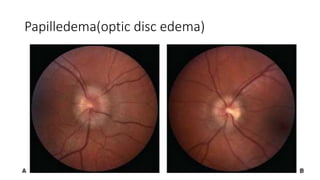
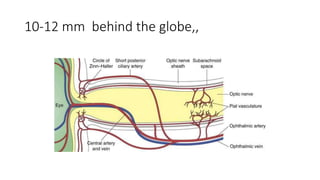
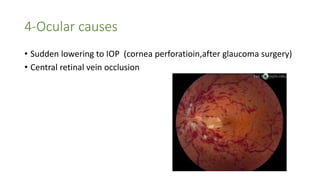

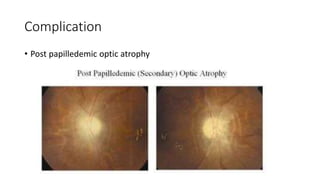
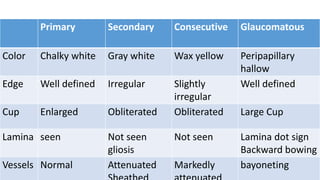
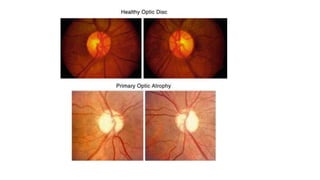
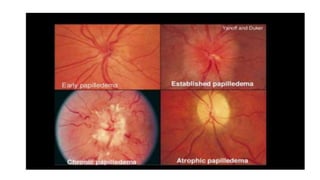
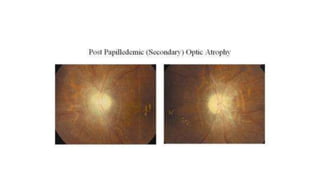
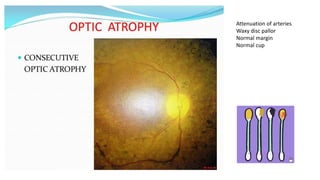
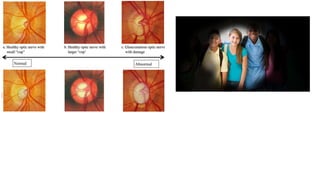
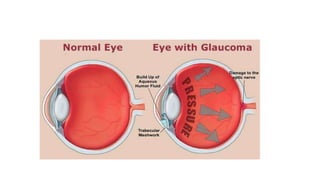
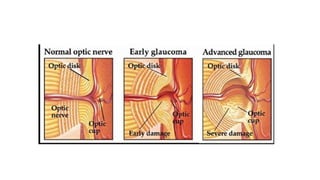
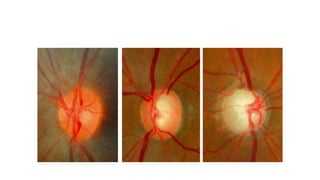
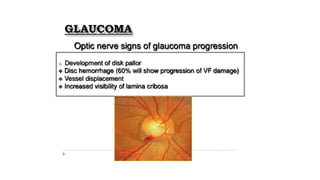

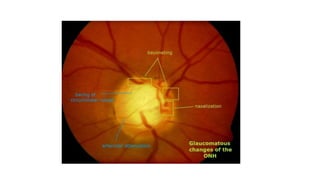
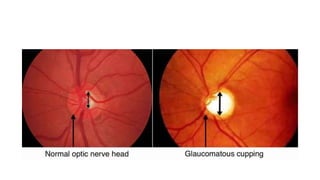
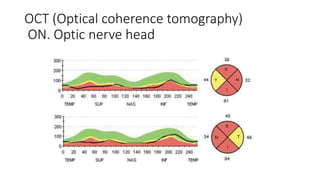
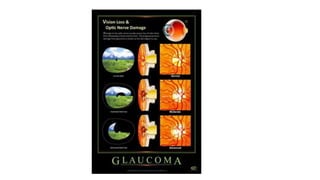
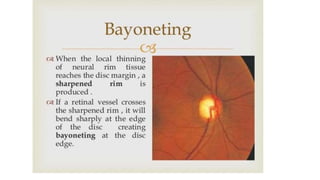
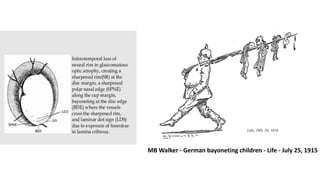
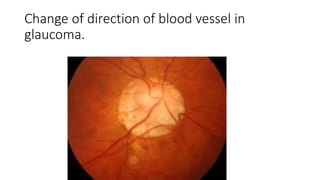


This document provides information on neuro-ophthalmology topics including mydriasis, miosis, causes of pupil changes, cervical sympathetic ganglia, medications that cause pupil changes, neurological causes of pupil changes, and optic nerve and disc topics. It discusses Horner's syndrome, Adie's pupil, optic disc edema/papilledema, optic atrophy including primary, secondary, consecutive, and glaucomatous types. It provides details on clinical presentation, investigations, complications, and characteristics of different types of optic atrophy. Images are included showing examples like Foster Kennedy syndrome, optic disc edema, optic atrophy, and retinal vessel changes in glaucoma.



















































































