INTRODUCTION:
• Normal discdiameter – 1.18-1.75 mm
• Disc area ranges from 0.68-4.42 mm2
• Disc area linearly increased by 1.2% +/- 0.15%
for each dioptre increase towards myopia(>-5D)
and decreased in hypermetropia (> +5D)
• A normal optic disc is vertically oval with the
vertical diameter being the maximum diameter
and the horizontal being the minimum diameter
3.
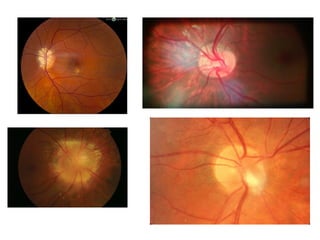
• Pseudopapilledema isdefined as anomalous
elevation of one or both optic discs without
edema of the retinal nerve fiber layer.
• Papilledema, on the other hand, is a swelling
of the optic disc due to increased intracranial
pressure
CAUSES OF PAPILLEDEMA:
•Expanding mass lesion (e.g. brain tumor)
• Cerebral edema due to stroke
• Intracranial hemorrhage
• Compression of the ventricular system in the
posterior fossa
• Venous sinus thrombosis
• Infectious etiology (e.g. cryptococcal meningitis)
• Pseudotumor cerebri
9.
• Causes ofbilateral optic disc edema without raised
intracranial pressure:
• Hypertensive emergency
• Diabetic papillopathy
• Toxic insult
• Metabolic or nutritional deficiency
• Optic perineuritis (caused by infectious or
inflammatory conditions)
• Other causes: optic neuritis, ischemia, compression
from orbital tumors
10.
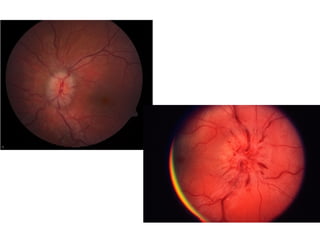
SIGNS OF DISCEDEMA:
• MECHANICAL SIGNS:
1.Elevation of the optic disc(3D=1mm)
2.Blurring of the disc margins
3.Filling in of optic cup
4.Edema of peripapillary nerve fiber
5.Retinal/choroidal folds
11.
• VASCULAR SIGNS:
1.Hyperemiaof disc
2.Venous congestion
3.Peripapillary hemorrhages
4.Exudates in disc/peripapillary area
5.Nerve fiber layer infarcts
12.
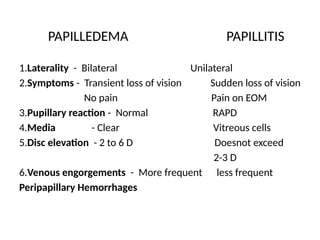
PAPILLEDEMA vs. PAPILLITIS
•Papilledema is bilateral,passiva,non-
inflammatory swelling of optic disc due to
raised intracranial pressure
• The main difference is visual acuity and optic
nerve function are normal in
papilledema,whereas it is disturbed in
papillitis
13.
PAPILLEDEMA PAPILLITIS
1.Laterality -Bilateral Unilateral
2.Symptoms - Transient loss of vision Sudden loss of vision
No pain Pain on EOM
3.Pupillary reaction - Normal RAPD
4.Media - Clear Vitreous cells
5.Disc elevation - 2 to 6 D Doesnot exceed
2-3 D
6.Venous engorgements - More frequent less frequent
Peripapillary Hemorrhages
2.Neuro-imaging:
-Urgent CT torule out space occupying lesions and CT
venogram to rule out cerebral venous malformations
-MRI MRV with contrast would assess for
leptomeningeal enhancement if meningitis was
suspected
-Lumbar puncture (to be done after neuroimaging
demonstrates no risk for herniation) to assess for
elevated opening pressure and signs infection or
inflammation (e.g., CSF cell count, protein, glucose)
17.
• If toxicor infectious etiologies are suspected,
then other laboratory or serologic testing may
be indicated.
• Further laboratory studies may include ESR,
CRP and CBC for inflammatory etiologies.
18.
TREATMENT:
• MEDICAL THERAPY:
1.Malignanthypertension-antihypertensive agents
2.Acetazolamide (contraindicated in cryptococcal
meningitis due to metabolic acidosis)
3.corticosteroid/immunosuppressive therapy-for
inflammatory etiology
4.High dose i.v corticosteroids,IVIG,plamapharesis-
demyelinating disease
5.Antibiotics-infective etiology
19.
• SURGERY:
-Intracranial masslesion-neurosurgical intervention.
-Persistent disc edema due to increased ICP not
responding to maximum medical therapy or that is
associated with acute vision loss at onset (e.g.,
fulminant IIH) require optic nerve sheath fenestration
and/or cerebrospinal fluid shunt device
- A lumbar drain may be necessary for papilledema in
the acute setting (eg, fulminant IIH) as a temporizing
measure prior to definitive surgical treatment.
20.
PROGNOSIS:
• With appropriateand prompt treatment, in
most cases vision can be preserved.
• Prolonged disc edema - increases the risk of
permanent nerve damage and vision loss.
• Patients with acute and severe disease at onset
(e.g., malignant hypertension or fulminant IIH)
require more urgent and aggressive
intervention for better long-term prognosis.
21.
Anterior ischemic opticneuropathy:
NON-ARTERITIC AION:
• Occlusion of short posterior ciliary arteries-
partial/total infarction of optic nerve head
• Age >50,but younger than those with AAION
• DM,APA
syndrome,hypertension,hyperlipidemia,sleep
apnoea
22.
Symptoms:
• Sudden painlessmonocular vision loss
Signs:
• Decreased VA
• Visual field defects
• Dyschromatopsia proportional to VA
• Diffuse/sectoral disc swelling with few splinter
hemorrhages(disc swelling gradually resolves)
23.
Investigations:
• BP monitoring
•Fasting lipid profile,blood glucose
• Neuroimaging in some cases
Treatment:
• No definitive treatment
• Short term steroid treatment
• Treating underlying cause
• Aspirin(doesnot prevent attack in fellow eye)
24.
ARTERITIC AION:
• Inuntreated cases of giant cell arteritis
• One-third develop fellow eye involvement within a
week
Symptoms:
• Sudden,profound unilateral vision loss preceded by
amaurosis fugax
• Periocular pain
• GCA symptoms-scalp tenderness,headache,jaw
claudication
• Diplopia
25.
Signs:
• Severe visionloss with altitudinal visual field defect
• Pale ‘chalky white’ edematous disc-suggesting GCA
• Swelling resolves gradually-severe OA ensues
Prognosis: very poor,permanent vision loss.partial
recovery with immediate systemic steroids
Pseudo-Foster Kennedy syndrome-consequence of
AION-active disease in one eye is associated with
contralateral optic atrophy in fellow eye due to
previous episode
26.
Treatment:
• Intravenous methylprednisolone500mg-1g/day for 3
days,oral prednisolone 1-2 mg/kg/day.After 3 more days-
oral dose reduced to 50-60mg/day for 4 weeks/until
symptoms resolution & ESR/CRP becomes normal
• Along with weekly bisphosphonate,calcium/vit D
supplementation
• Monitoring by physician for steroid-related complications
• Antiplatelet therapy with aspirin 600mg stat then
100mg/day
• Methotrexate –in cases of steroid resistance
27.
ONTT
• The OpticNeuritis Treatment Trial (ONTT) was a randomized trial that
evaluated the value of corticosteroids in the treatment of acute optic neuritis
• •3-day course of methylprednisolone given intravenously in a dose of 250 mg
every 6 hours followed by 2 weeks of daily oral prednisone in a dose of 1
mg/kg/day accelerated visual recovery but did not improve the eventual
visual outcome
• •Treatment with oral prednisone alone in a dose of 1 mg/kg/day for 2 weeks
also did not improve visual outcome and was associated with an increased
rate of optic neuritis recurrences
• An unexpected finding was that those who received intravenous
corticosteroids followed by oral corticosteroids had a temporarily reduced risk
of development of a second demyelinating event consistent with MS over the
first two years compared with subjects who received oral corticosteroids
alone or placebo
28.
MACULAR EDEMA:
• Anatomy:round area in posterior pole,lying
inside temporal visual arcade,measuring 5-6
mm in diameter,subserves central 15-20
degree of the visual field,shows more than 1
layer of ganglion cells,contains xanthophyll
carotenoid pigments lutein & zeaxanthin
29.
Cystoid macular oedema:
•Accumulation of fluid in outer plexiform &
inner nuclear layers with cyst-like cavities
• Accumulate initially in muller cells then
rupture
• Small cavities coalesce-foveal lamellar hole
with irreversible central vision impairment
• CMO is non-specific manifestation of variety
of causes
Diagnosis:
• Symptoms-blurring ofvision,micropsia,distortion
• Signs-loss of foveal depression,thickening of
retina,multiple cystoid areas,optic disc
swelling,lamellar hole may be visible,features of
associated disease
• Amsler chart-central blurring,distortion
• FA-petaloid pattern due to dye accumulation in cystic
spaces
• OCT-retinal thickening with cystic hyporeflective
spaces and loss of foveal depression.lamellar hole in
advanced cases
32.
DIABETIC MACULAR EDEMA:
•Diffuse retinal edema due to extensive
capillary leakage & localised oedema by focal
leakage from microaneurysms and dilated
capillary segments
• Fluid initially located between outer plexiform
& inner nuclear layer.later may involve inner
plexiform and nerve fibre layer,until entire
thickness becomes odematous
33.
Focal maculopathy-well-circumscribed retinal
thickeningwith complete/incomplete ring of
exudates.FA shows focal hyperfluorescence
due to leakage with good macular perfusion
Diffuse maculopathy-diffuse retinal thickening
associated with cystoid changes.typically with
scattered MA & small hemorrhages.FA shows
mid-late phase diffuse hyperfluorescence
34.
Clinically significant macularedema: detected
clinically
• Retinal thickening within 500 micrometres of the
center of macula
• Exudates within 500 micrometres of the center of
macula,if associated with retinal
thickening(thickening itself maybe outside the
500 micrometres)
• Retinal thickening one-disc area(1500
micrometre) or larger,any part of which is within
one-disc diameter of the centre of macula
35.
• Microcystic macularedema:
• Microcystic changes of the inner nuclear layer
distinct from classic CMO can occur in eyes
with optic neuritis and some other forms of
optic neuropathy. It is believed to be caused
by retrograde degeneration of the inner
retinal layers that manifests with impaired
fluid resorption.
36.
• • Treatmentof macular oedema. Treatment is
generally indicated for VA worse than 6/9
and/or with significant central macular
thickening (e.g. >250 µm) on OCT, but is
unlikely to be of benefit if 6/120 or worse.
• Intravitreal anti-VEGF agents
• Intravitreal dexamethasone implant





















































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)












