Downloaded 390 times









![HIGH QUALITY Cpr
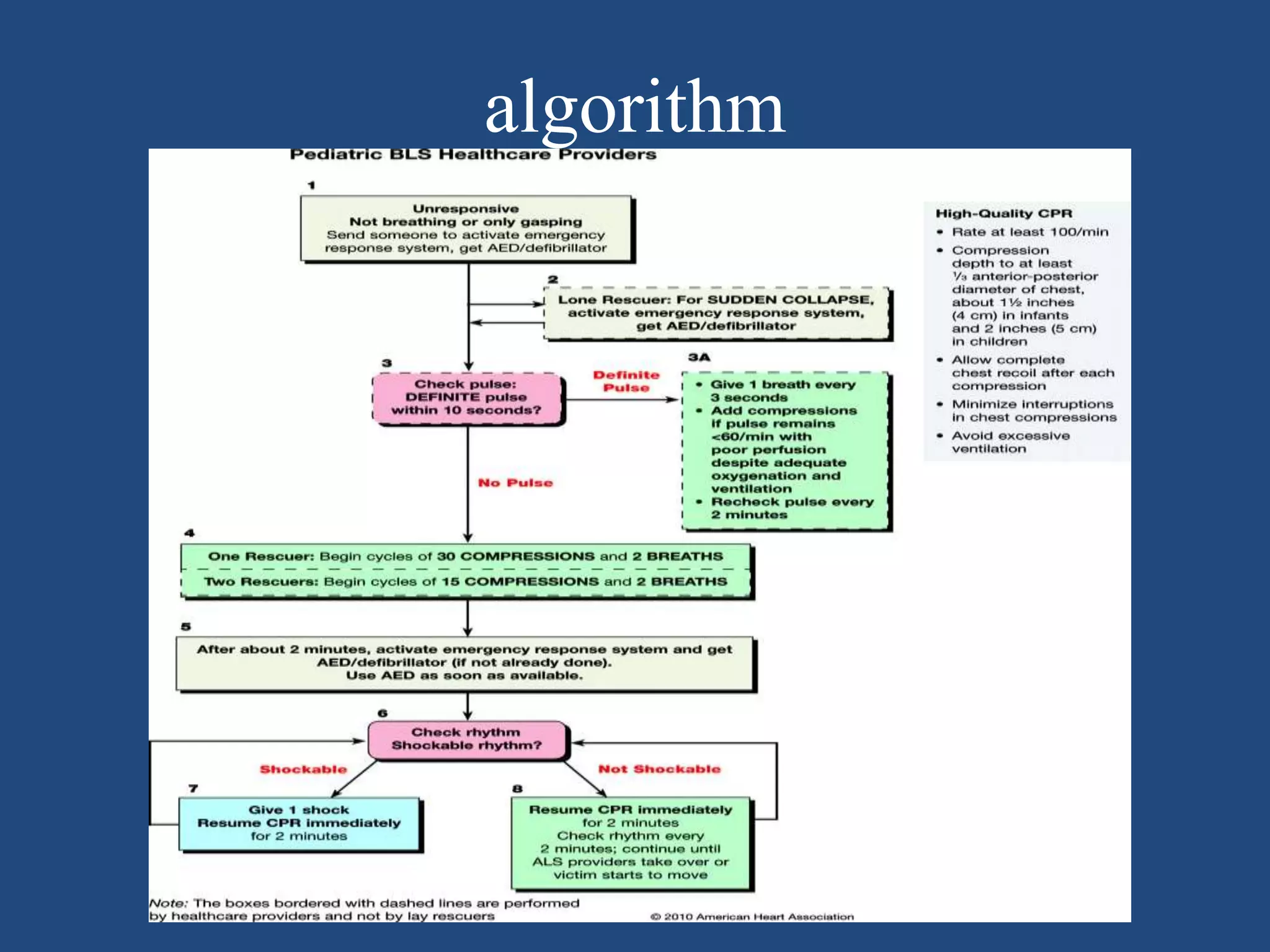
S tart COMPRESSION within 10 seconds of recognition of arrest
P USH HARD ,PUSH FAST :
Rate at least 100/min
Depth at least 5 cm in child and 4 cm for infants
Complete chest Recoil
Minimize Interruptions
Give effective Breathing
Avoid excessive ventilation
Cycle : 5 cycles of [30:2] in approximately 2minutes. Recheck
for signs of life at the end of cycle
Ratio : 30 compression to 2 ventilation for 1 rescuer
: 15 compression to 2 ventilation for 2 rescuer](https://image.slidesharecdn.com/paediatricbls-171220190017/75/Paediatric-bls-13-2048.jpg)





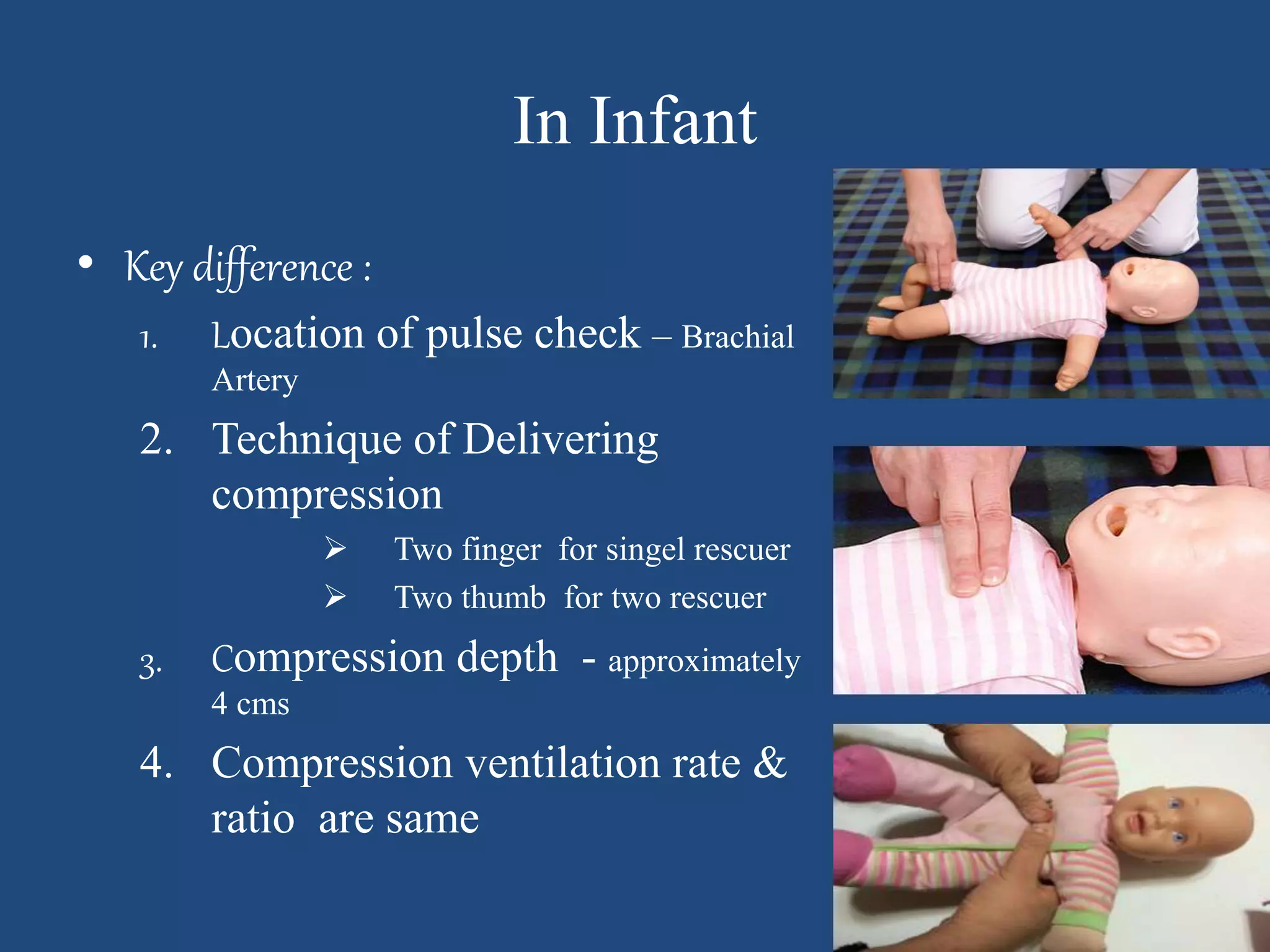

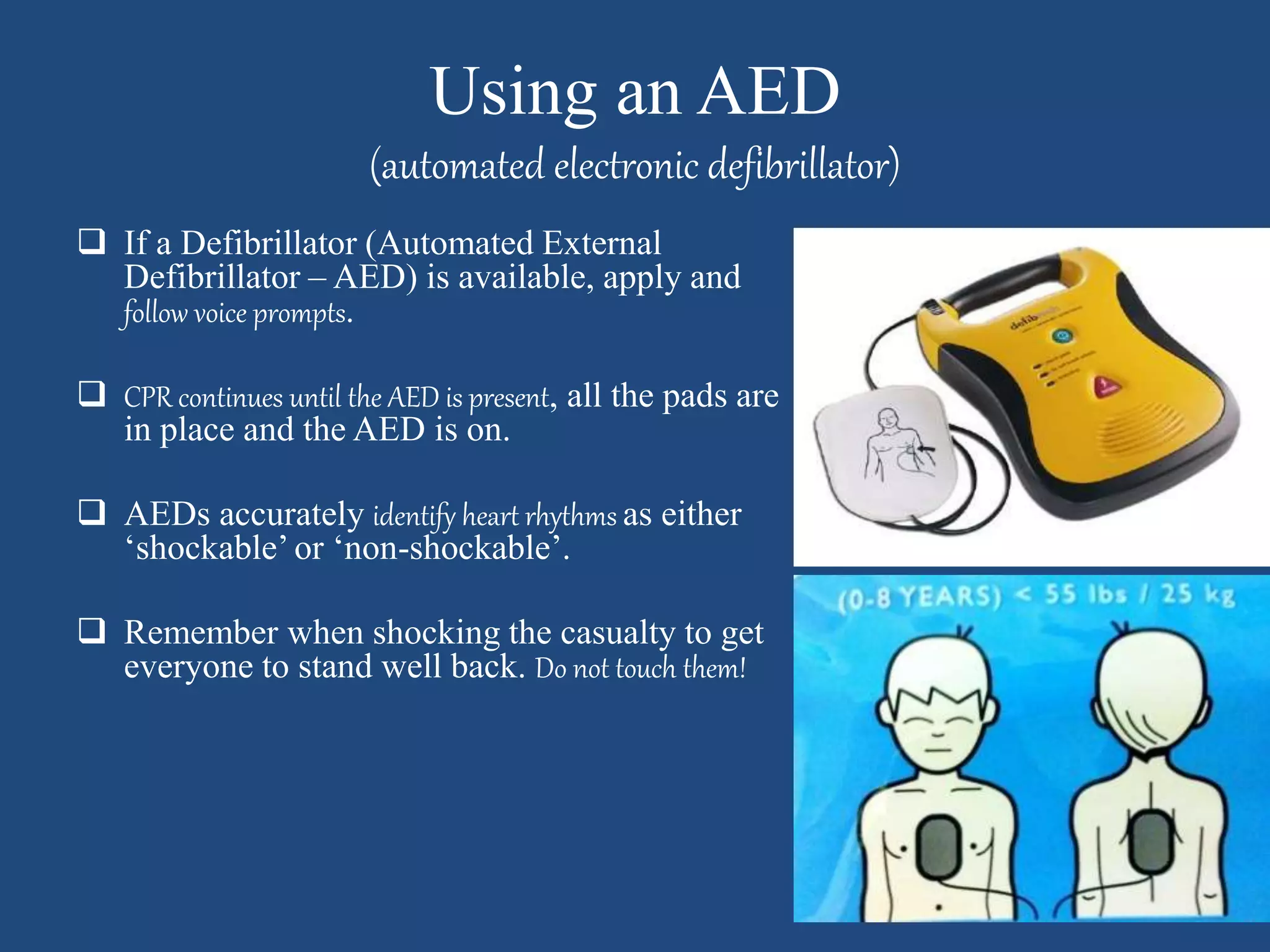





This document provides guidelines for paediatric basic life support. It outlines the key differences in caring for children compared to adults in emergency situations. The guidelines cover safety, response, calling for help, chest compressions, airway management, rescue breathing, and use of an automated external defibrillator. Emphasis is placed on high quality chest compressions and minimizing interruptions to compressions.























































































