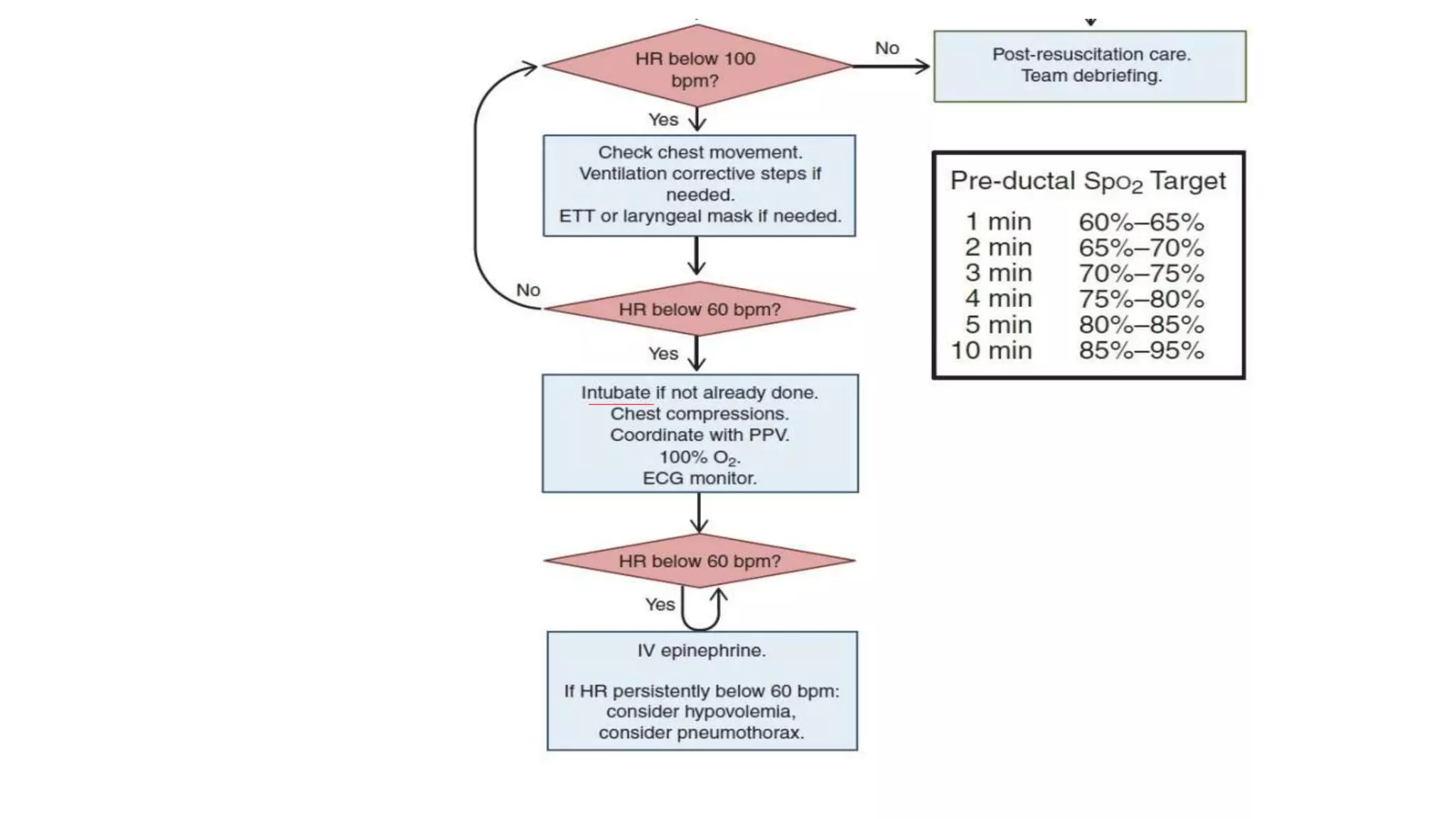
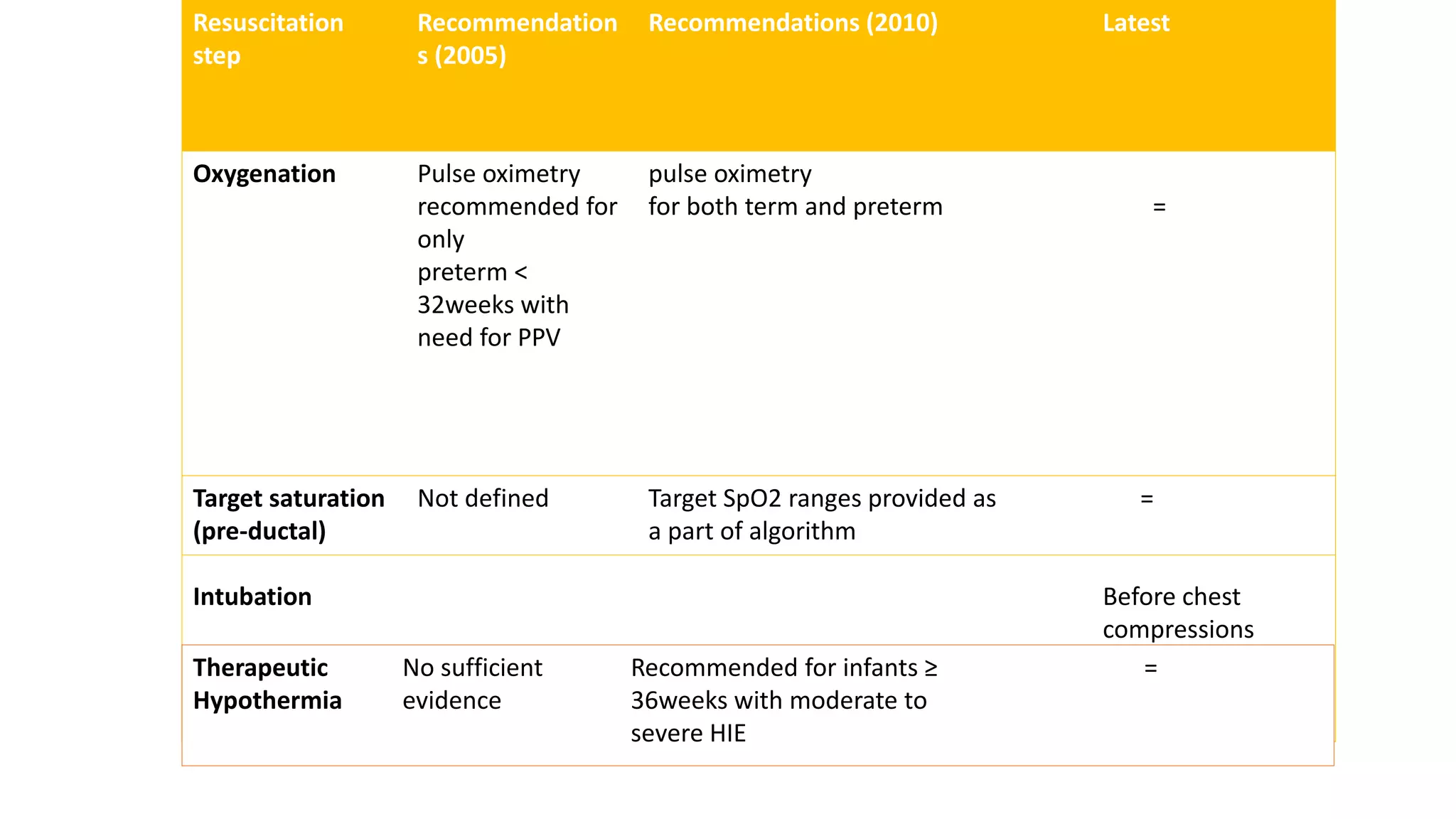
The document summarizes the key changes in neonatal resuscitation practices between the 2010 and 2016 guidelines. It highlights increased focus on team preparation and communication. Initial assessment and steps remain unchanged, but temperature control during resuscitation is emphasized. Pulse oximetry is now recommended for both term and preterm infants to guide oxygen use. Intubation should now occur before chest compressions. Therapeutic hypothermia is recommended for infants 36 weeks or older with hypoxic-ischemic encephalopathy.