Downloaded 121 times
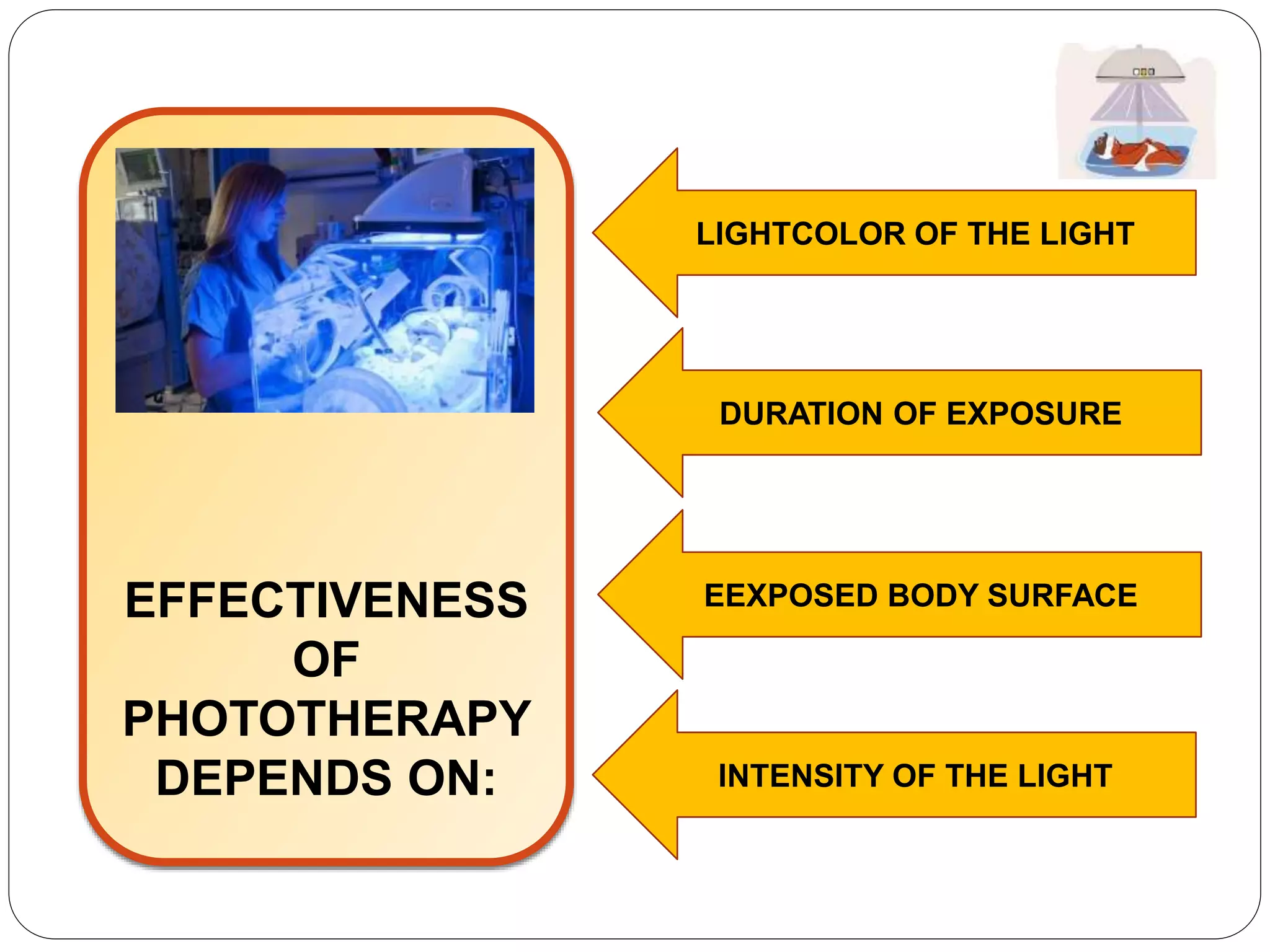


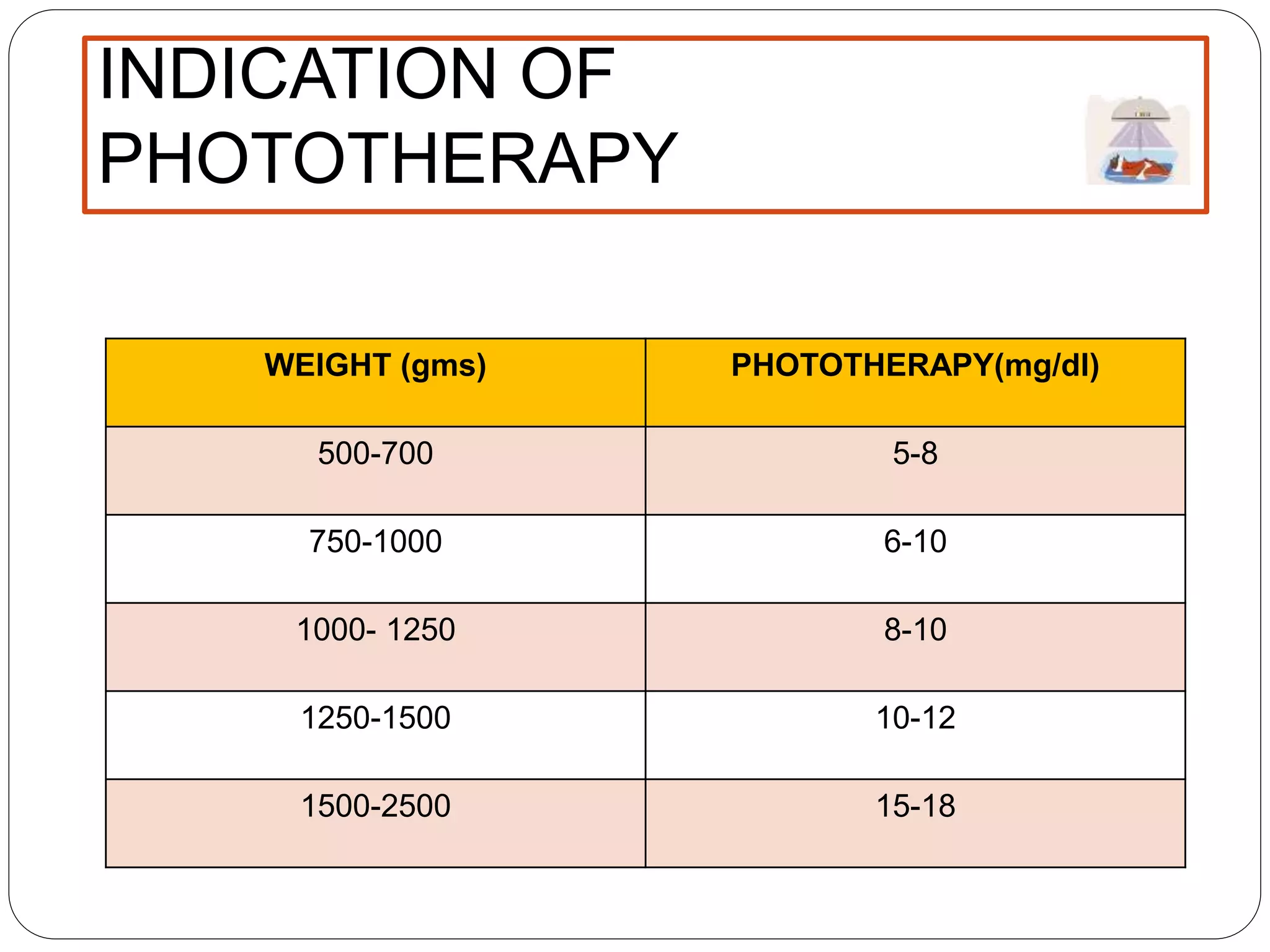


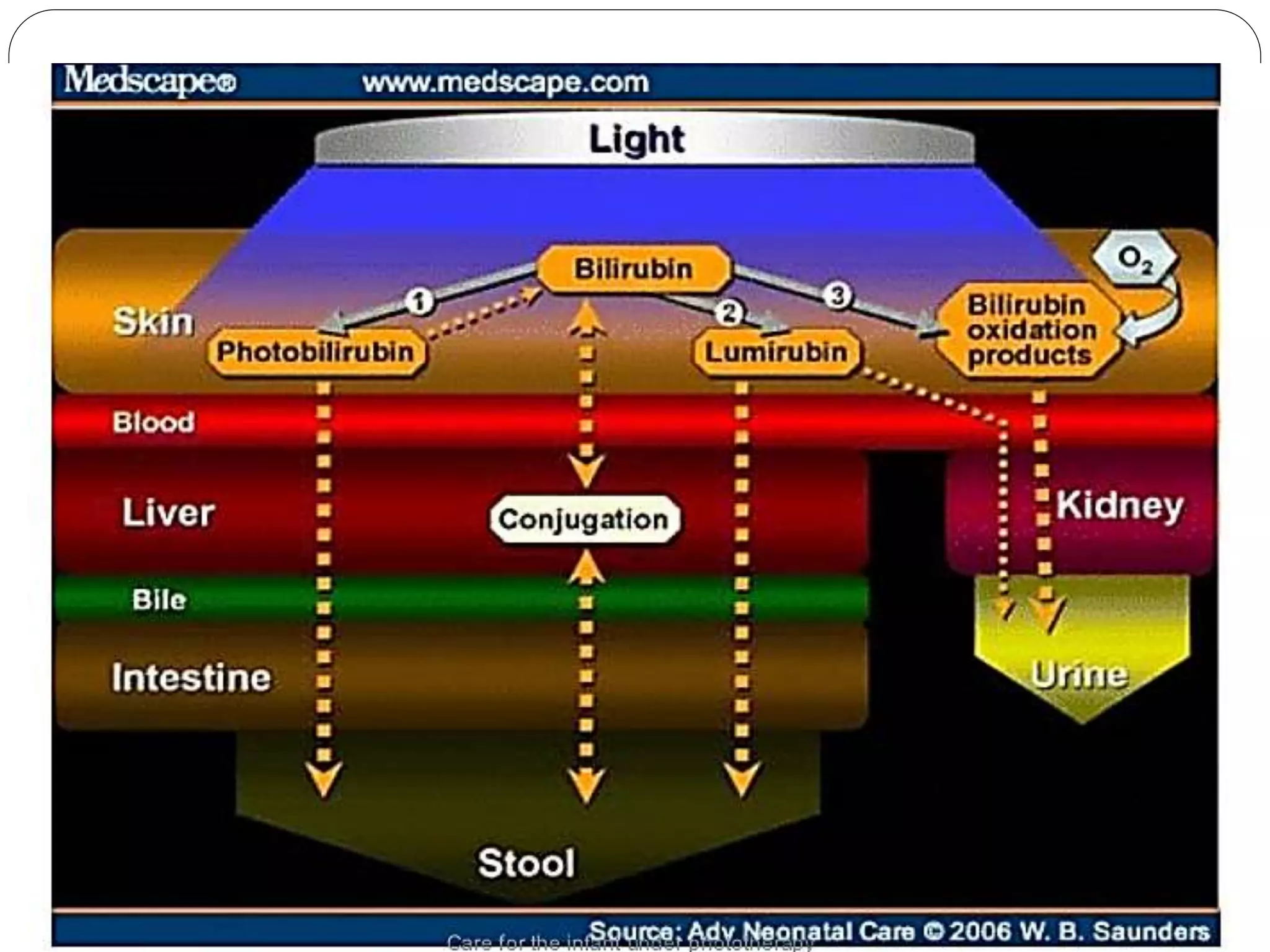








Phototherapy is a treatment for neonatal hyperbilirubinemia that uses specific light wavelengths (400-500 nm) to convert unconjugated bilirubin into a water-soluble form for excretion, preventing serious conditions such as acute bilirubin encephalopathy. It aims to lower bilirubin levels in infants, requiring careful monitoring of exposure, temperature, and fluid intake while minimizing separation from the mother. Nursing care includes managing skin integrity, hydration, and supporting parental involvement during treatment.