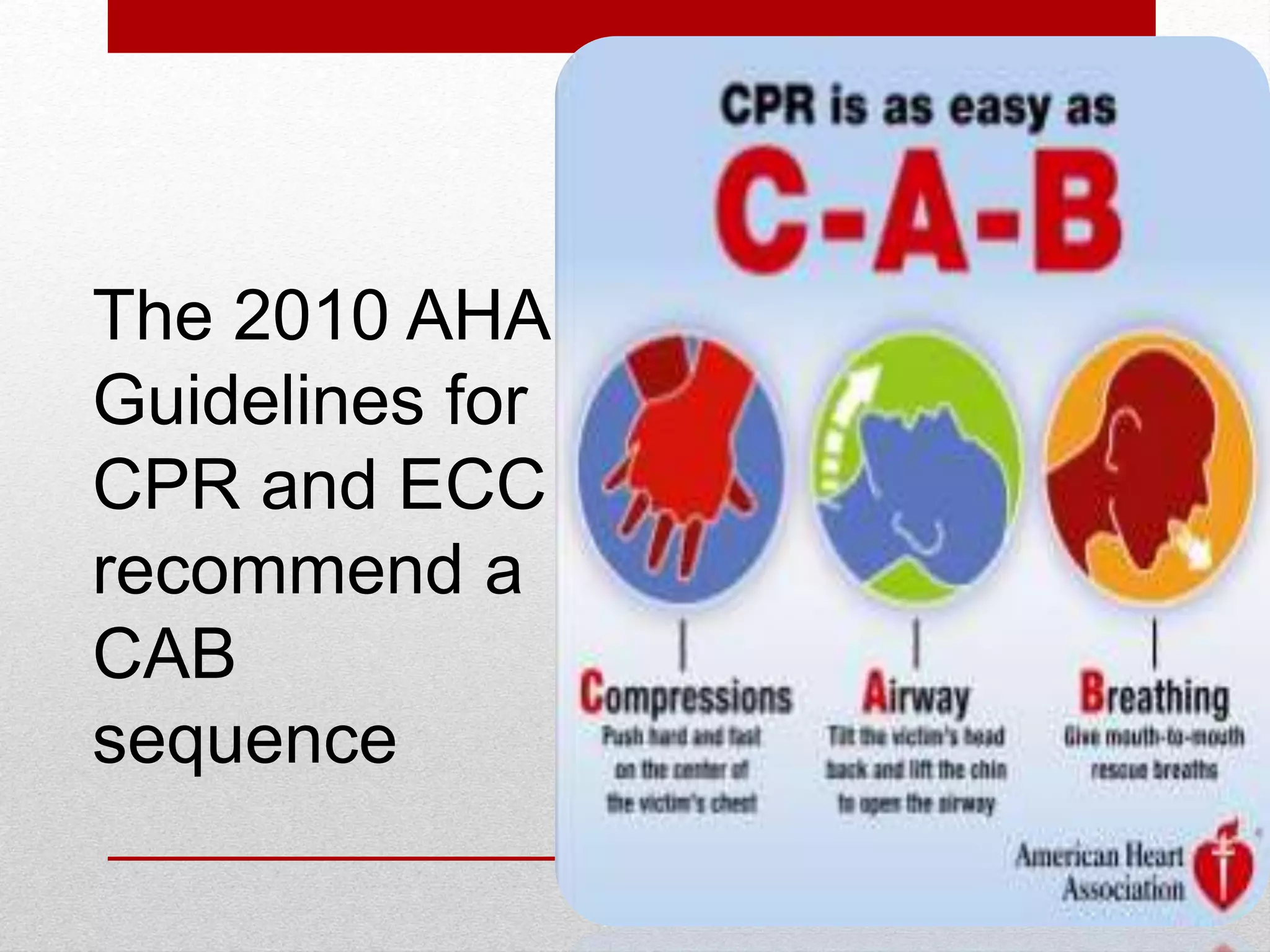
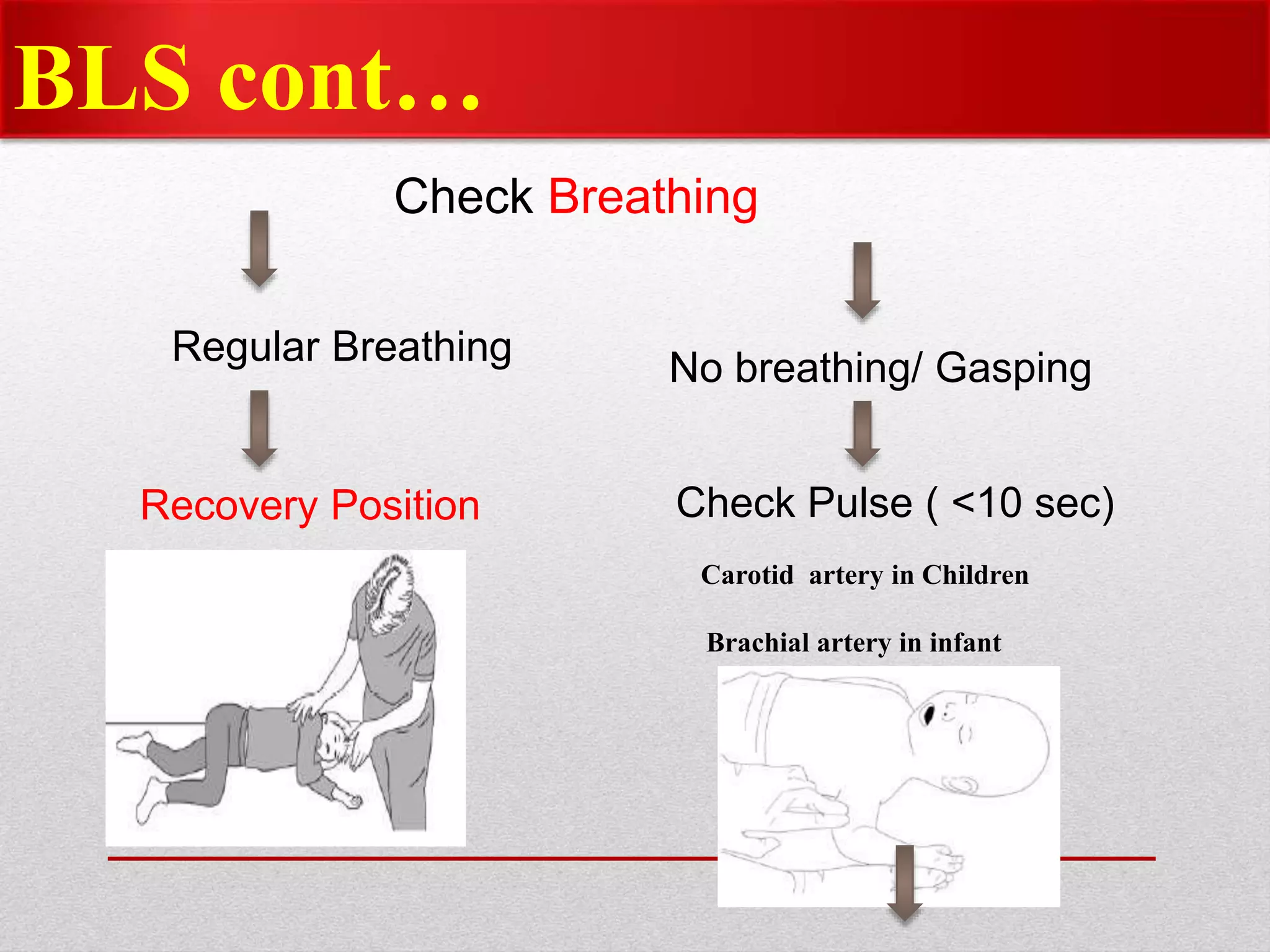
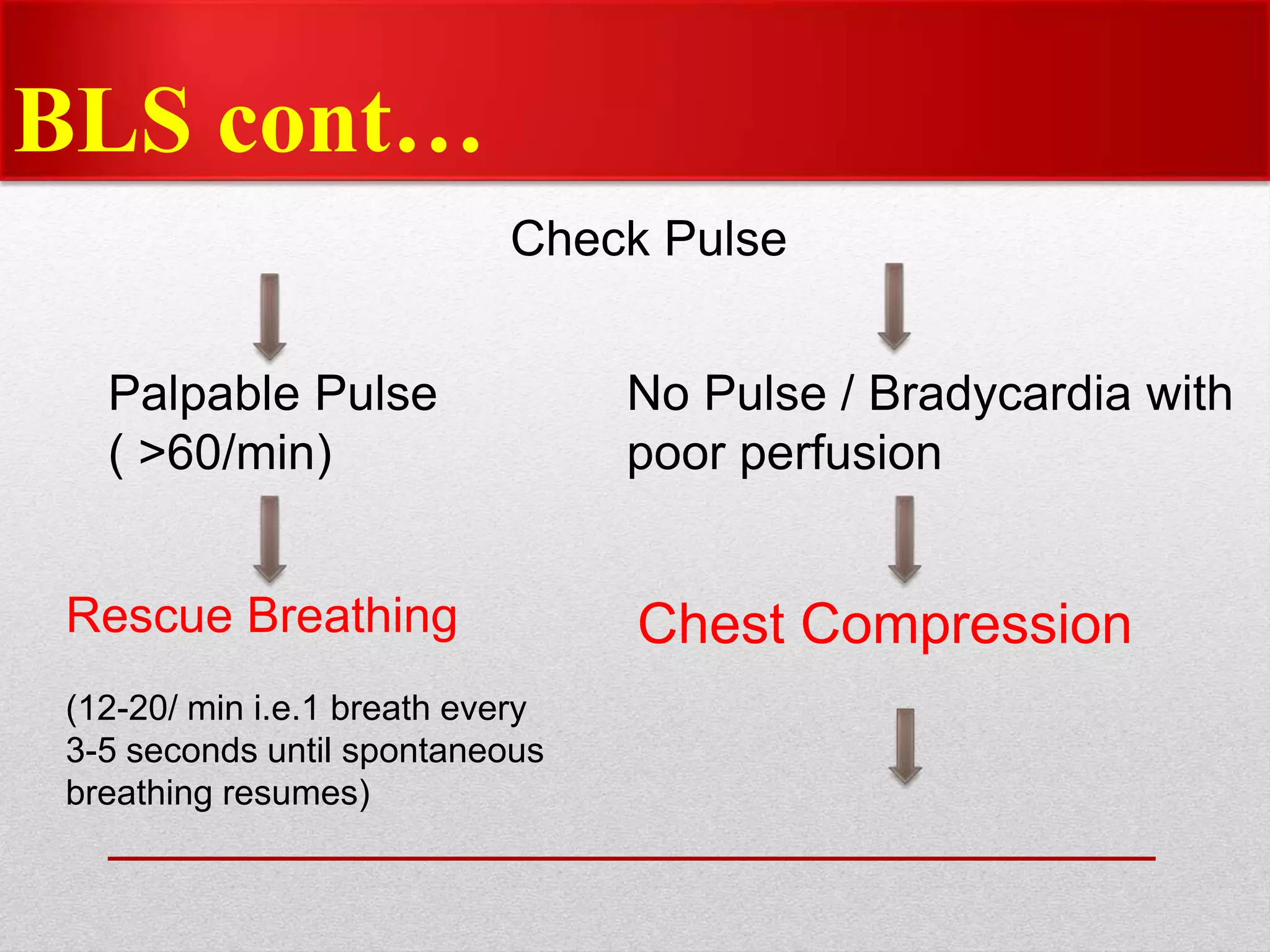
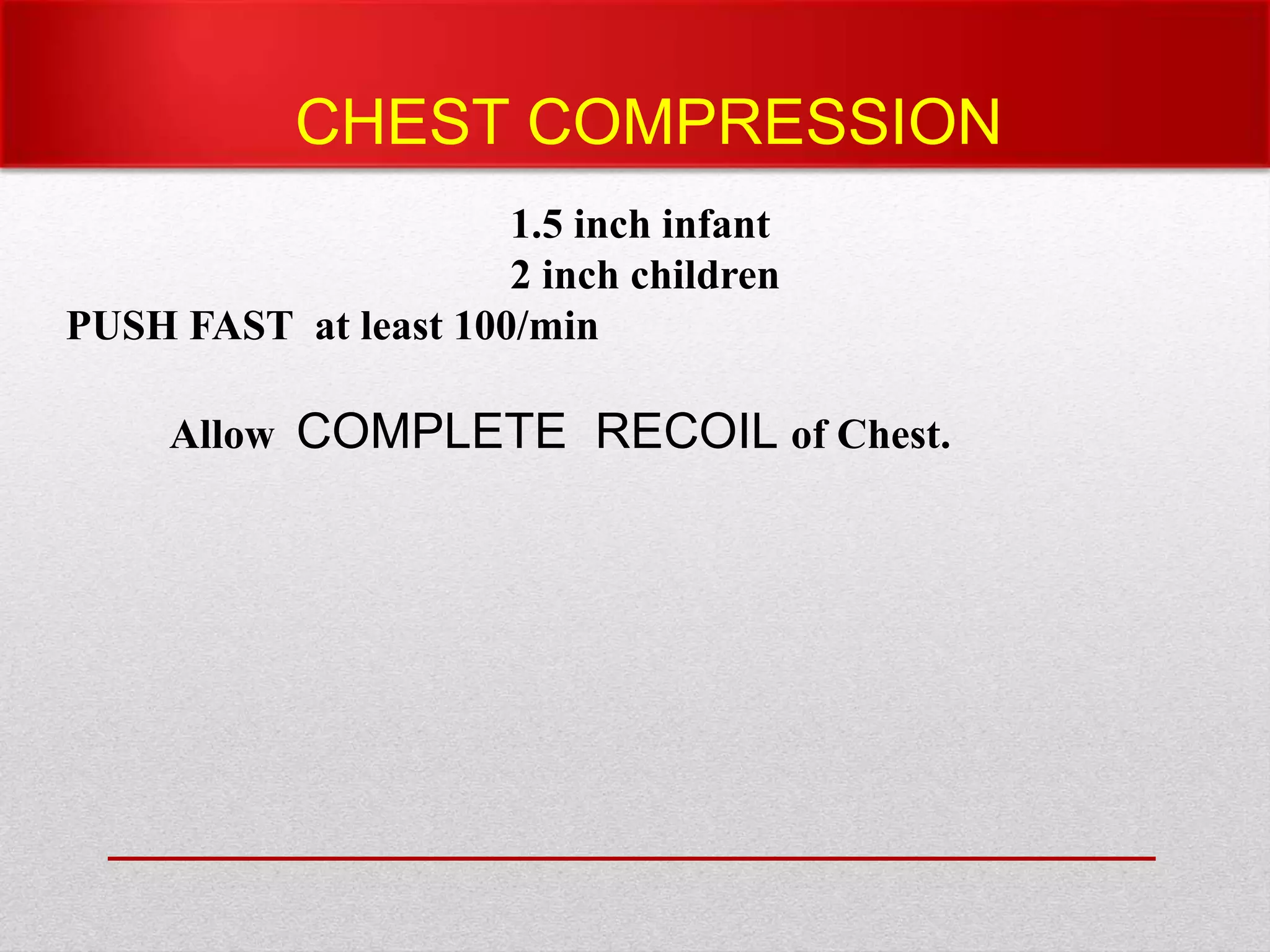
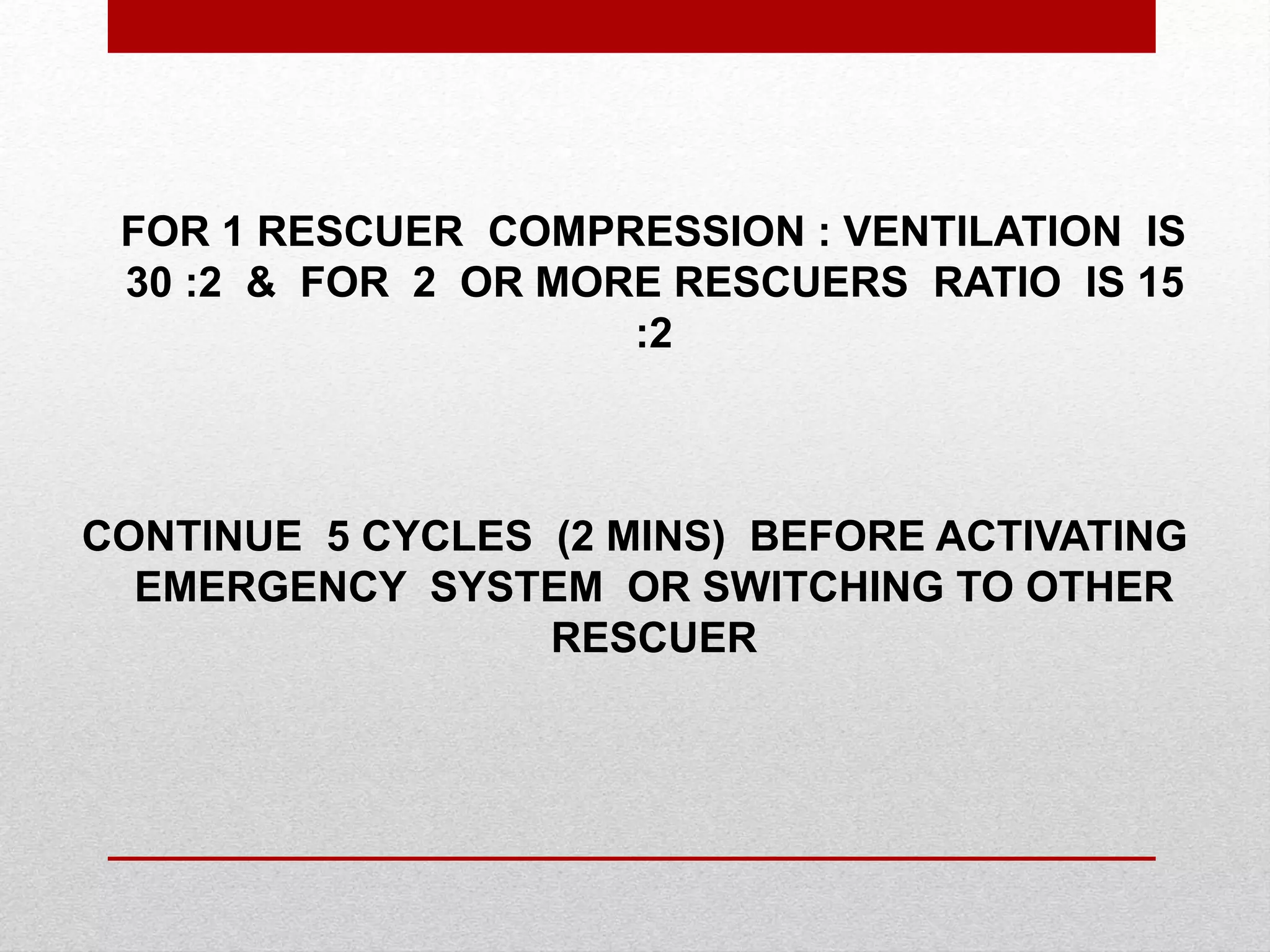
Paediatric basic life support (PBLS) involves resuscitation procedures to prevent anoxic brain damage and promote circulation and breathing in children. The key steps of PBLS are CAB - checking for circulation (C) by feeling for a pulse, opening the airway (A), and giving rescue breaths (B). For infants and children in cardiac arrest, high-quality chest compressions at least 100/min that depress the sternum 1/3 its depth are critical, along with proper head positioning and rescue breathing. PBLS should continue for 2 minutes in cycles of 30 compressions to 2 breaths before emergency help arrives or switching rescuers.











































































![MEDICAL EMERGENCIESinpd [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/medicalemergenciesautosaved-241228041041-66b7393f-thumbnail.jpg?width=640&height=640&fit=bounds)



![CPR AND EMERGENCY MEDICATIONS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cprandemergencymedicationsautosaved-250204082316-1c1ad7d9-thumbnail.jpg?width=640&height=640&fit=bounds)























