Download to read offline









































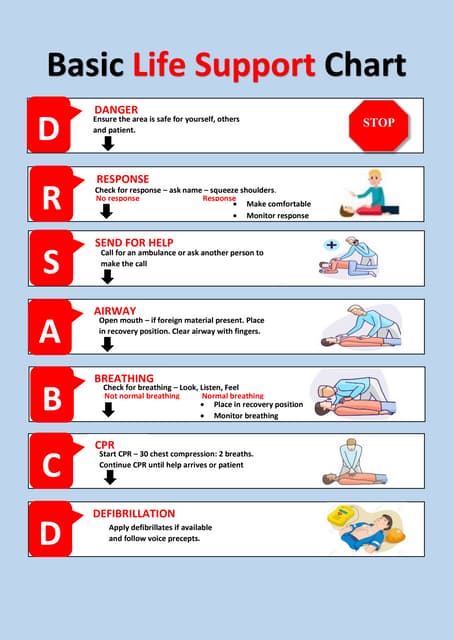
This document provides a comprehensive overview of Basic Life Support (BLS) protocols, including CPR techniques, the use of an AED, and choking interventions for both adults and infants. It emphasizes the importance of immediate action during cardiac arrest and defines circumstances for initiating or withholding CPR. The text details specific steps for performing high-quality CPR, including compression techniques and ratios, as well as considerations for different age groups and conditions.