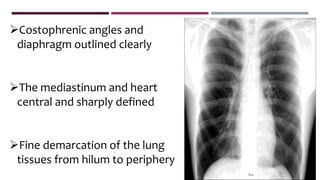
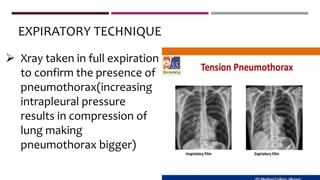
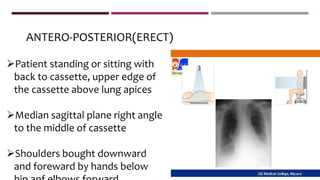
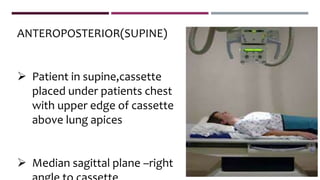
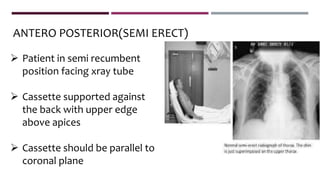
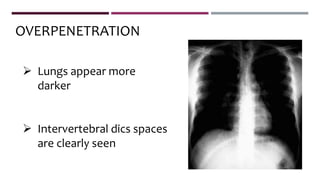
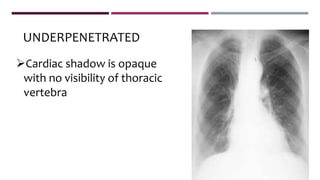
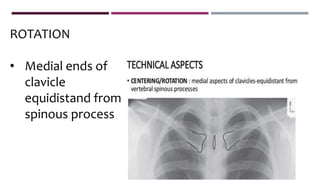
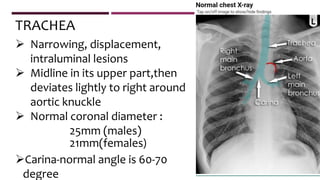
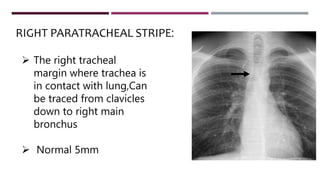
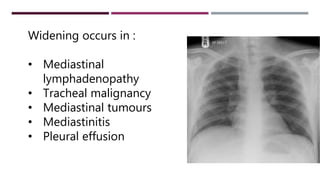
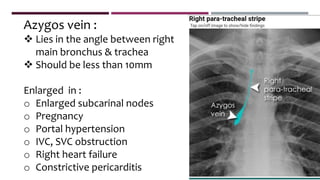
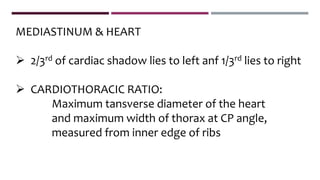
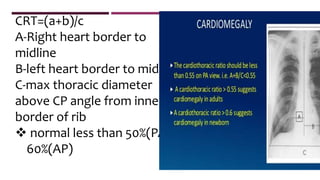
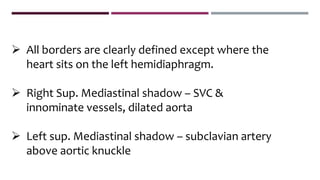
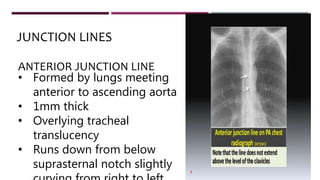
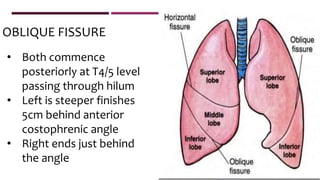
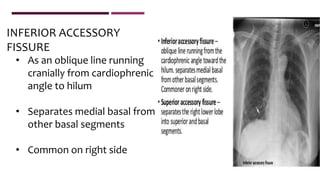
This document provides guidelines for performing and interpreting a normal chest x-ray. It describes recommended projections including PA, AP, lateral, and oblique views. Proper positioning, centering, penetration, and rotation are discussed. Key anatomical structures are defined, such as the mediastinum, heart, lungs, fissures, hila, and diaphragm. Common variations and pathological findings are outlined. The document aims to serve as a reference for radiologists in evaluating and diagnosing chest x-ray images.