Downloaded 26 times
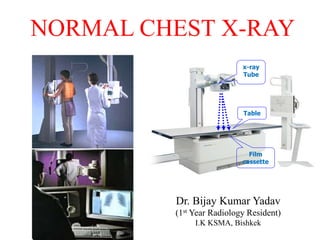
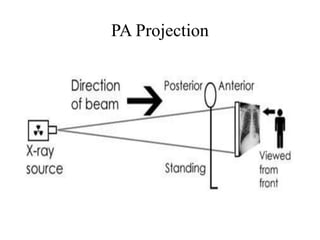
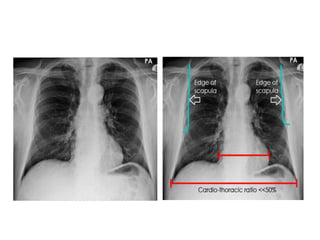
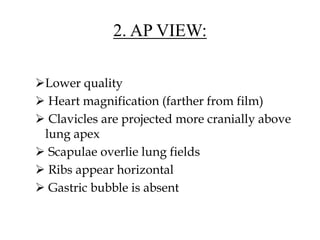
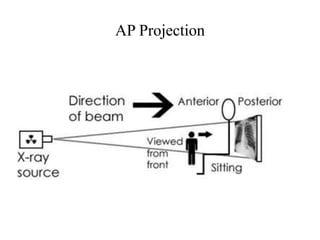
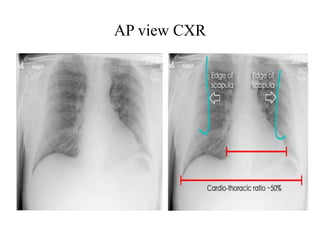
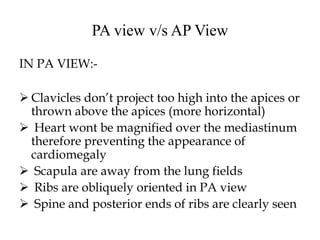
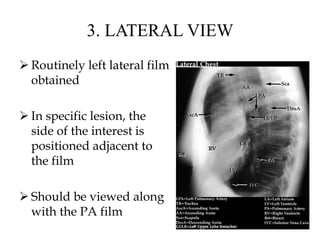
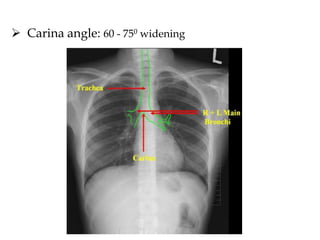
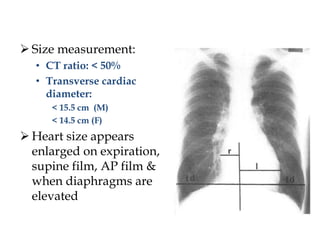
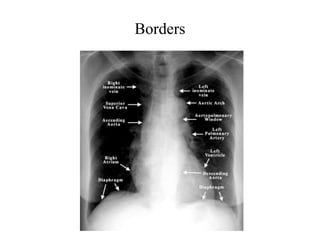
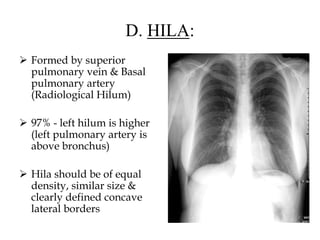



This document provides an overview of how to interpret a normal chest x-ray. It describes the key anatomical structures visible in a chest x-ray like the lungs, heart, diaphragm and bones. It explains how to assess technical aspects such as inspiration level. Common views taken are described including PA, AP and lateral views. A systematic approach is outlined starting with the trachea and moving through each area of the chest. Key anatomical variations and measurements are also defined.























































































