Downloaded 568 times
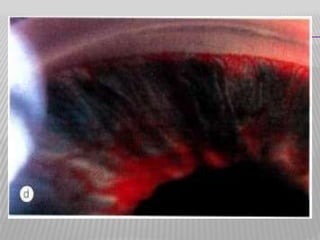
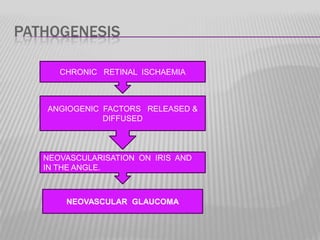
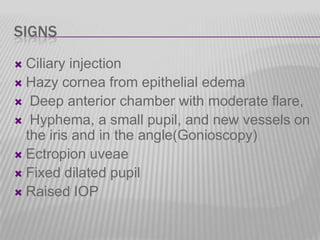
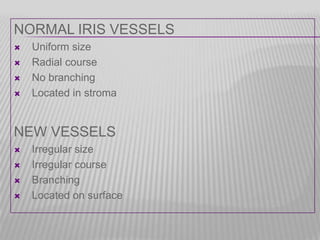
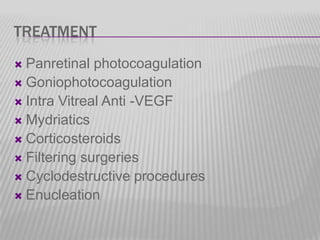
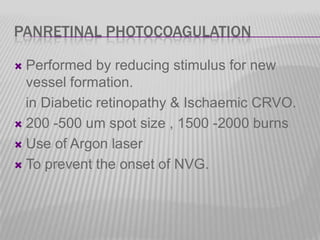


Neovascular glaucoma is a secondary glaucoma caused by the growth of new blood vessels on the iris and in the anterior chamber angle due to underlying retinal ischemia or disease. The new vessels are stimulated by hypoxic factors and can contract, pulling the iris forward and occluding the drainage angle. This leads to increased eye pressure and vision loss if not treated. Treatment options aim to reduce the stimulus for new vessel growth such as panretinal photocoagulation laser or anti-VEGF injections, lower eye pressure through filtration surgeries or cyclodestructive procedures, and manage pain.































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











