Downloaded 74 times
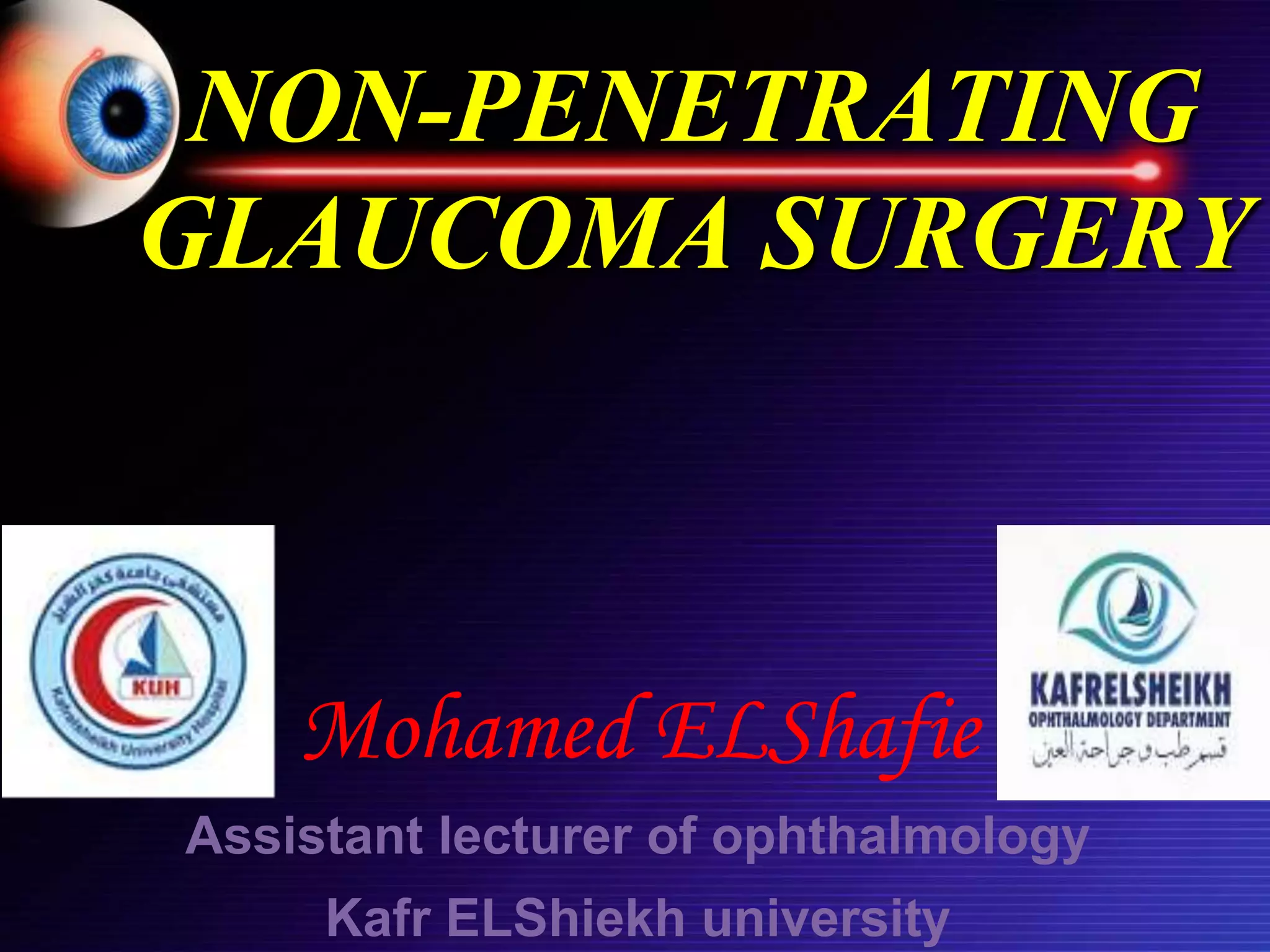
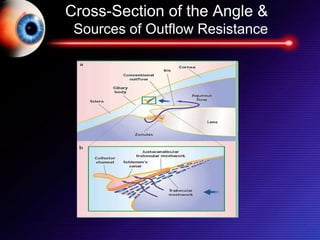

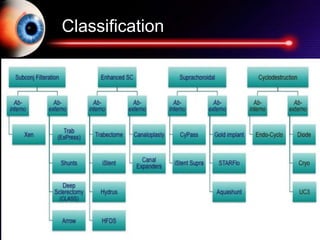
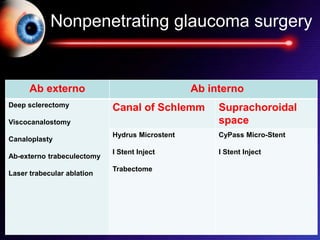
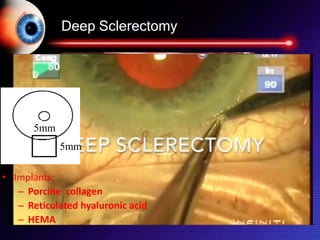



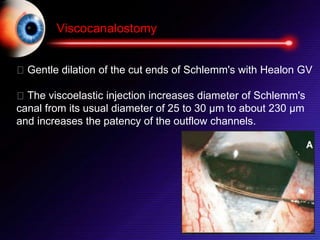
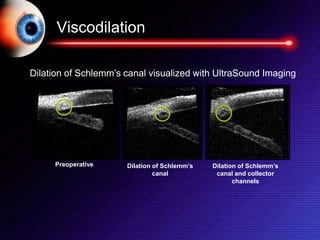


This document discusses non-penetrating glaucoma surgery techniques that facilitate the drainage of aqueous humor through the trabecular meshwork and Schlemm's canal without opening the anterior chamber. It describes several procedures including deep sclerectomy, viscocanalostomy, canaloplasty, ab-externo trabeculectomy, and laser trabecular ablation. The goal is to bypass the highest resistance point to outflow in the juxtacanalicular meshwork. Advantages include lower risks of complications like hypotony compared to penetrating surgeries. Indications and contraindications are provided for various non-penetrating glaucoma procedures.























































































