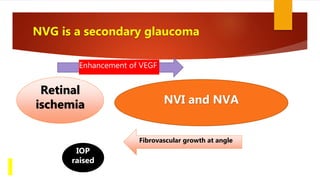
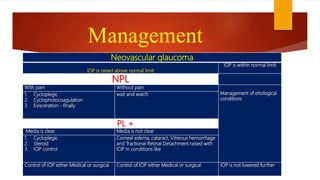
Neovascular glaucoma (NVG) is a secondary glaucoma caused by new blood vessel growth in the eye. It develops as a result of retinal ischemia which leads to the proliferation of fibrovascular tissue that obstructs the outflow of aqueous humor, increasing intraocular pressure. The main causes of retinal ischemia include diabetic retinopathy, central retinal vein occlusion, and ocular ischemic syndrome. Treatment involves reducing retinal ischemia through panretinal photocoagulation or anti-VEGF injections, controlling intraocular pressure through medications or surgery, and treating any underlying systemic diseases contributing to retinal hypoxia. While aggressive treatment can help prevent vision loss, NVG has a guarded prognosis, especially if intraocular pressure cannot be adequately

![Nomenclature history of NVG
Rubeosis iridis was first described by Coats with CRVO in
1906.[1]
This condition was called previously by different names such as
1. Rubeotic glaucoma
2. Diabetic hemorrhagic glaucoma
3. Congestive glaucoma
4. Thrombotic glaucoma
In 1963 Weiss et.al named it as Neo Vascular Glaucoma
in relation NVI and rise in IOP](https://image.slidesharecdn.com/neovascularglaucomapp1-220730021532-f6dc4c05/85/Neovascular-Glaucoma-pptx-4-320.jpg)


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






