Downloaded 753 times

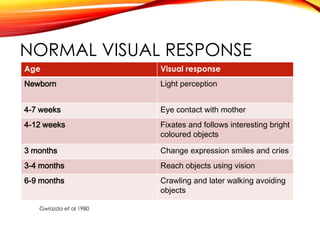
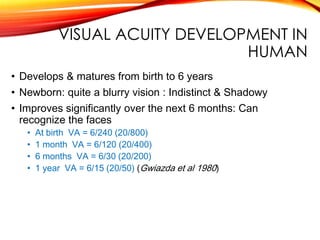
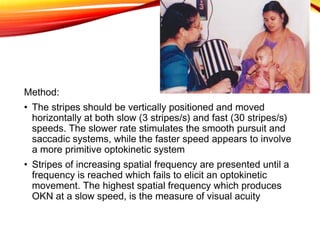
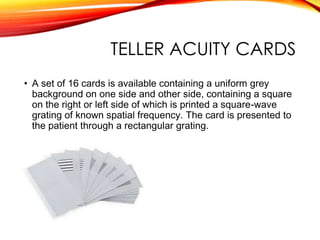
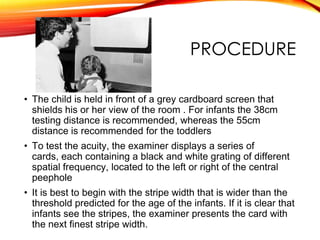
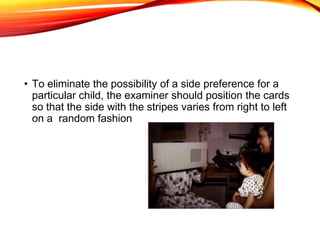
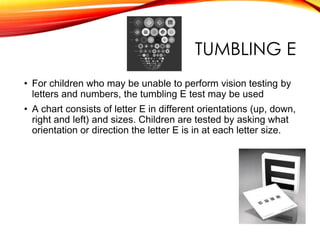
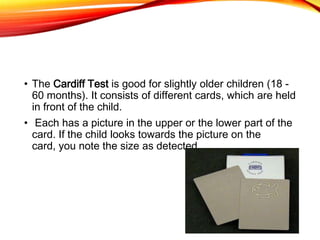


This document discusses methods for assessing visual acuity in pediatric patients. It begins by defining visual acuity and describing its normal development from birth through age 6. It then outlines different techniques for measuring various types of visual acuity, including detection, resolution, and recognition acuity. These techniques include methods that elicit voluntary responses like candy beads, as well as involuntary responses like optokinetic nystagmus drums and visual evoked potentials. Preferential looking tests using cards with different grating frequencies are described as a way to measure resolution acuity in nonverbal children.











































































































