Downloaded 12 times
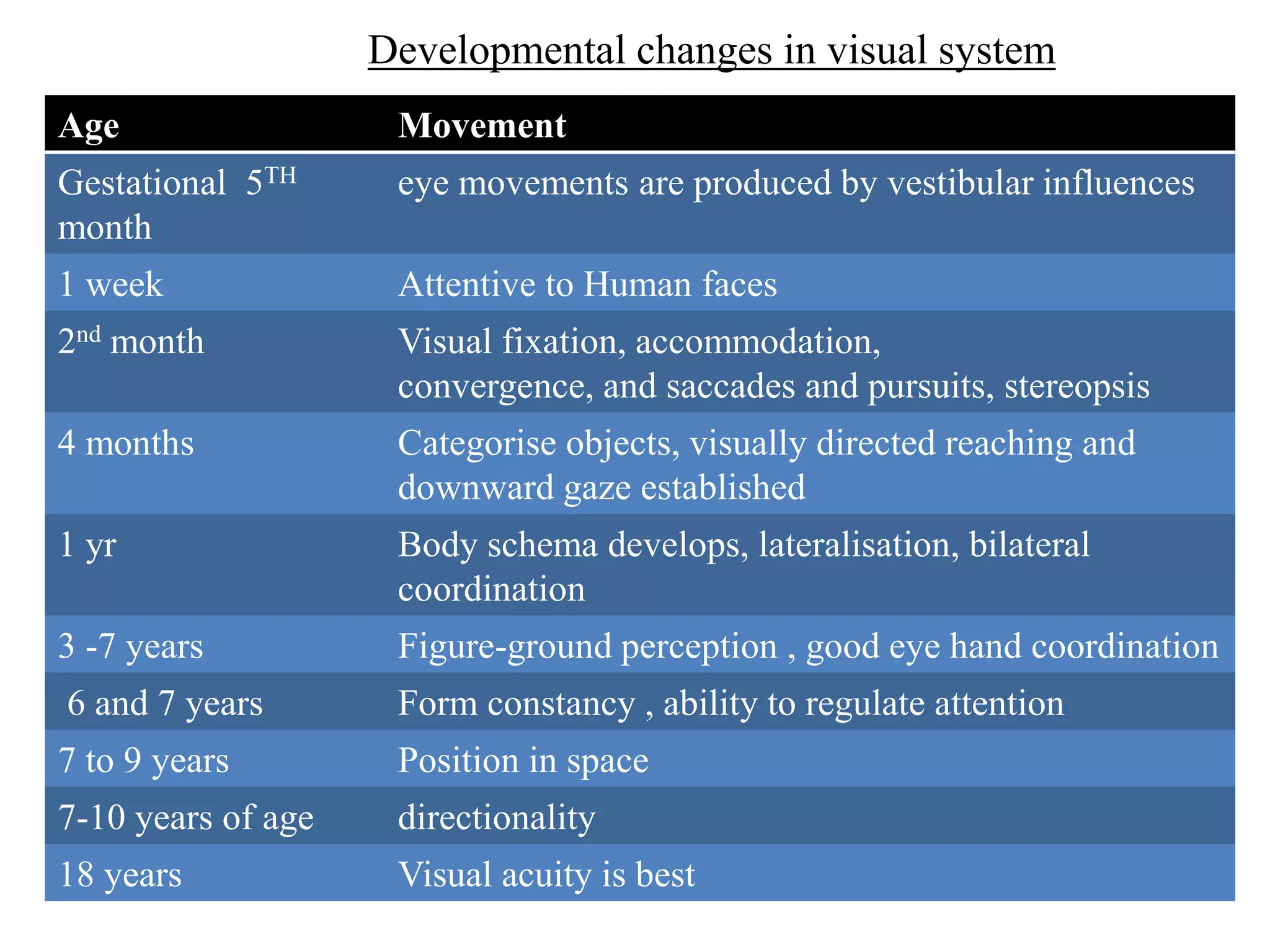
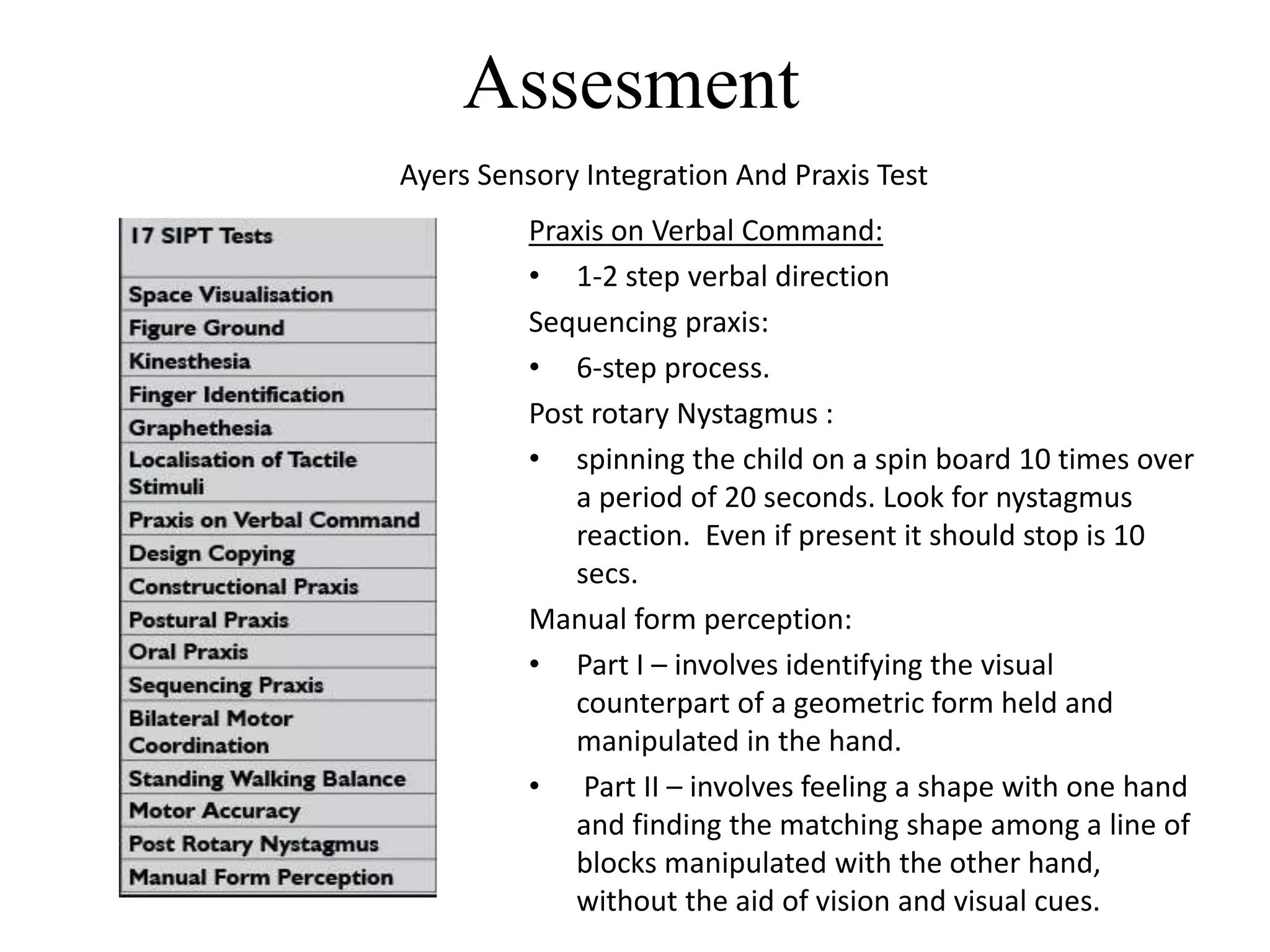
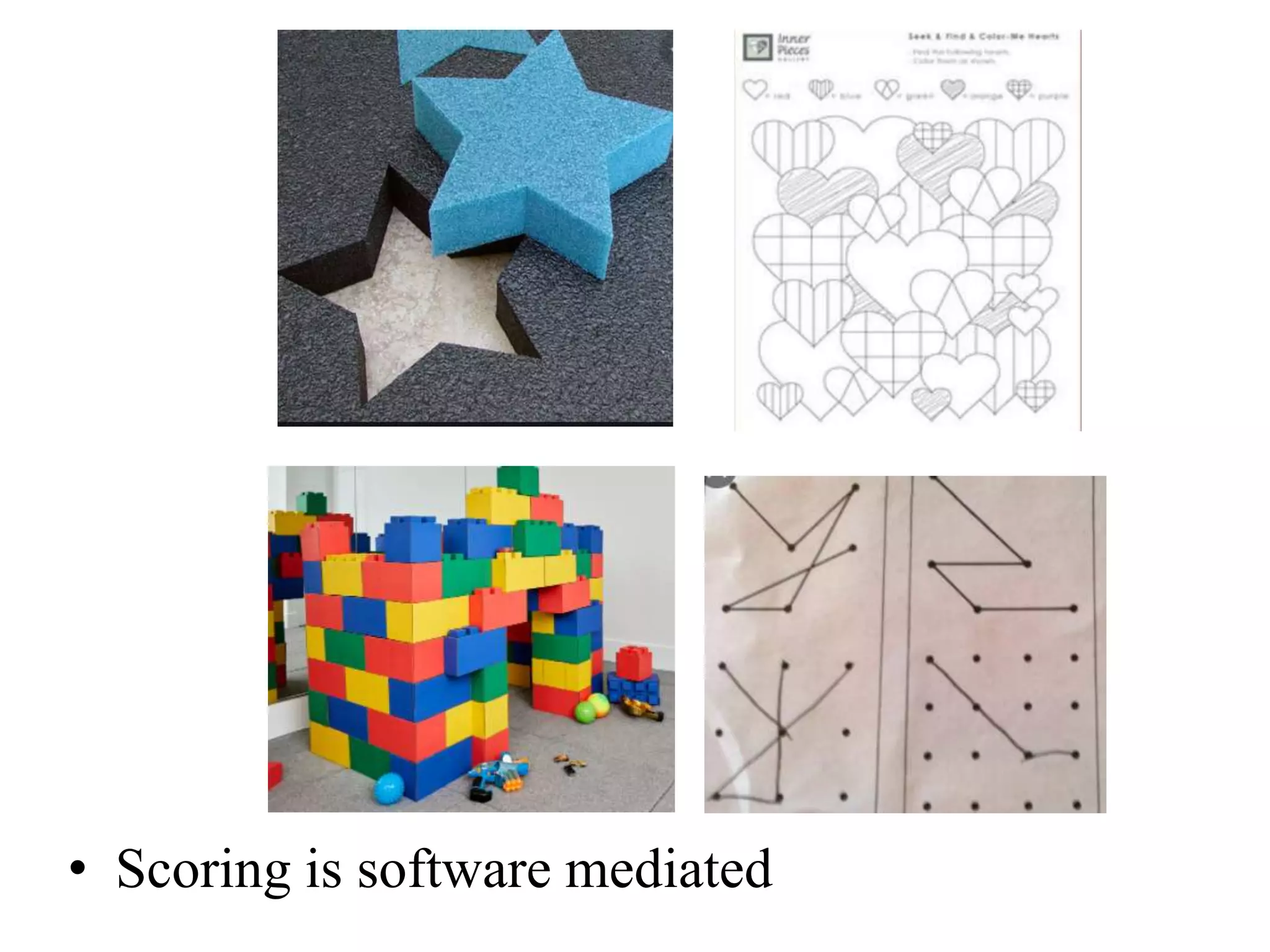
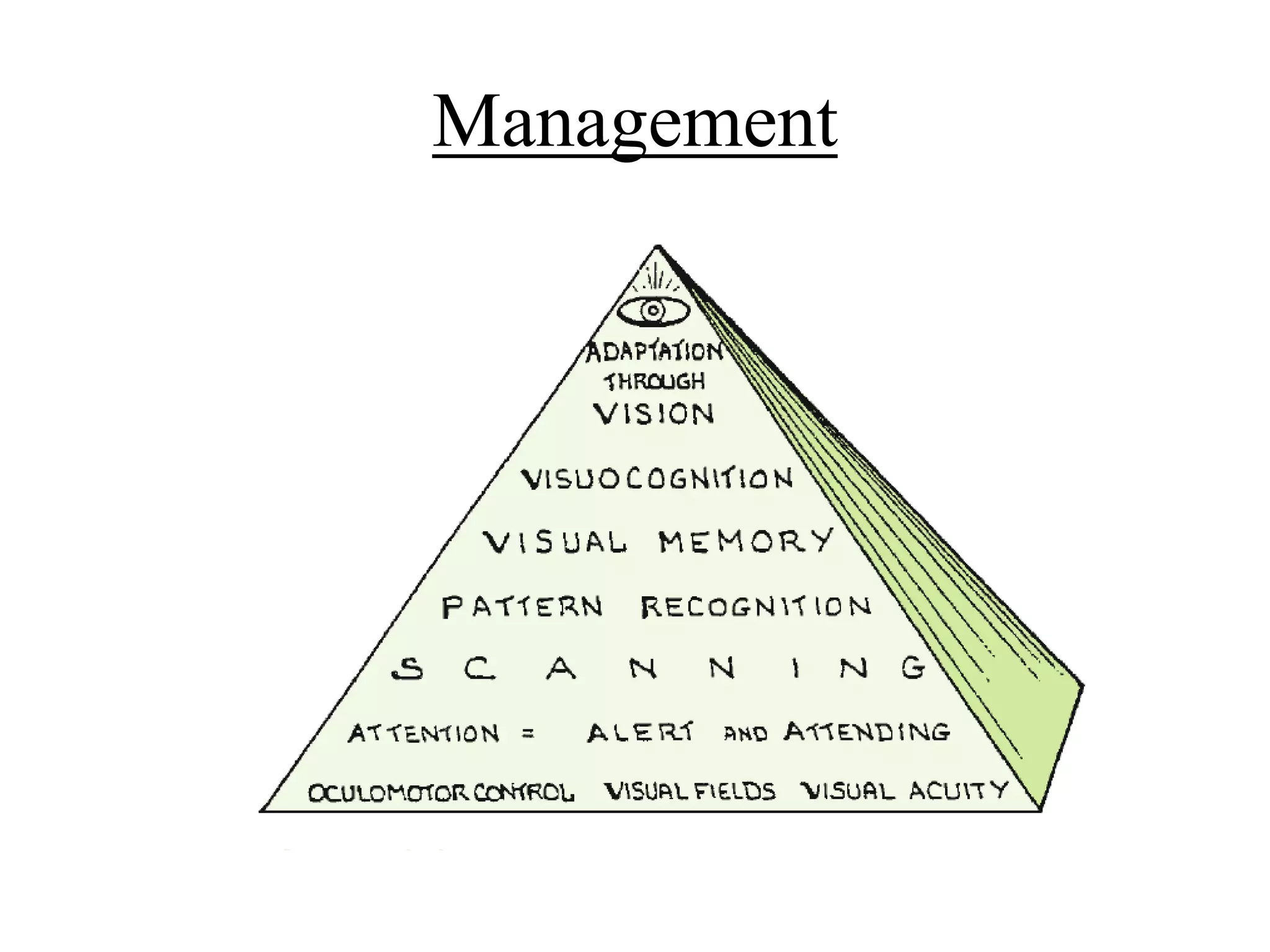


The document discusses visual perception, outlining its components, pathways, and functions including visual cognition and sensory integration. It highlights developmental milestones in visual functions and the impact of sensory modulation on visual processing, as well as management strategies for children with visual-motor integration challenges. Additionally, it presents a study on augmented biofeedback training improving visual-motor integration in children with spastic hemiplegia, detailing methods, results, and implications for therapy.