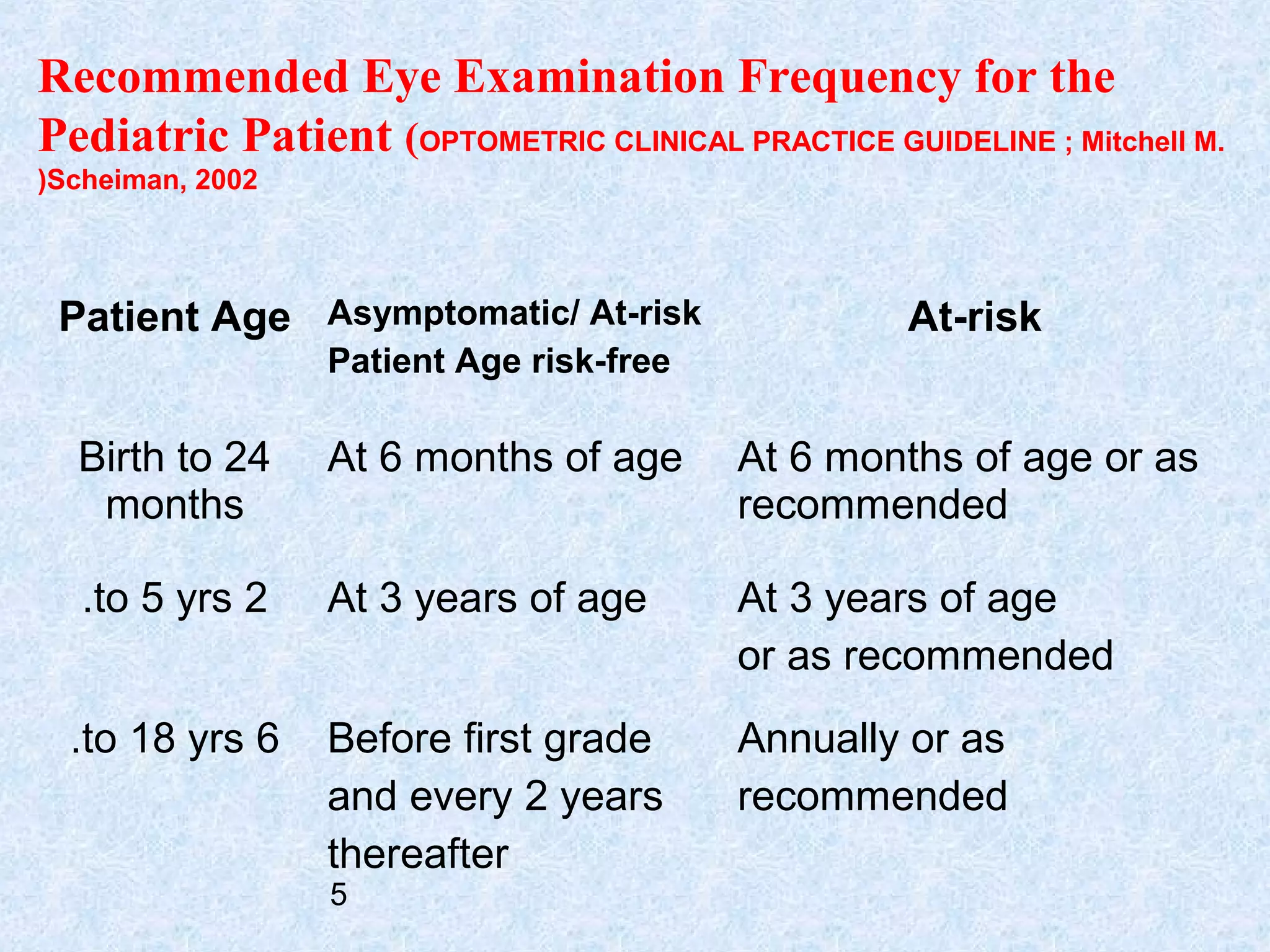
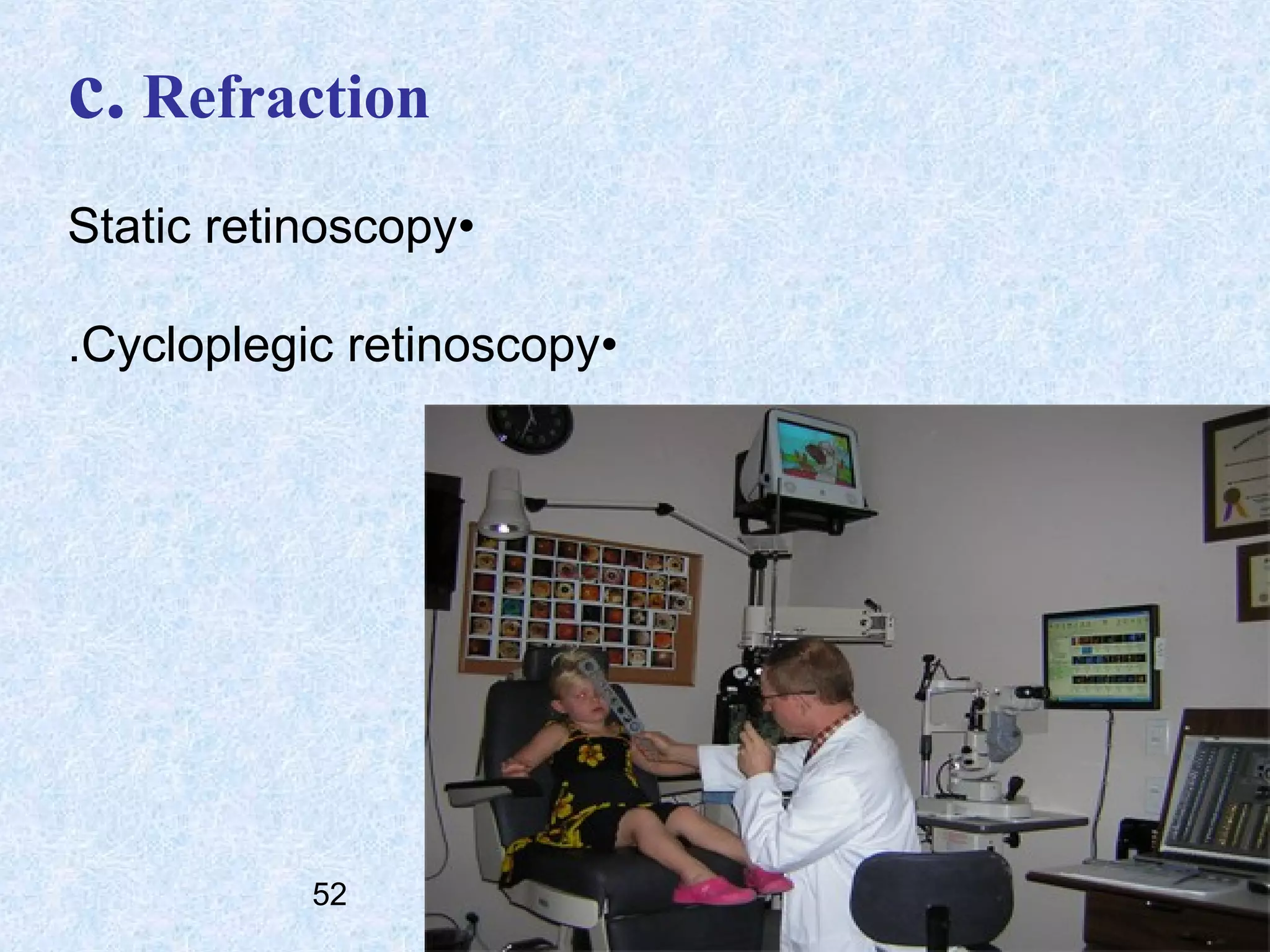
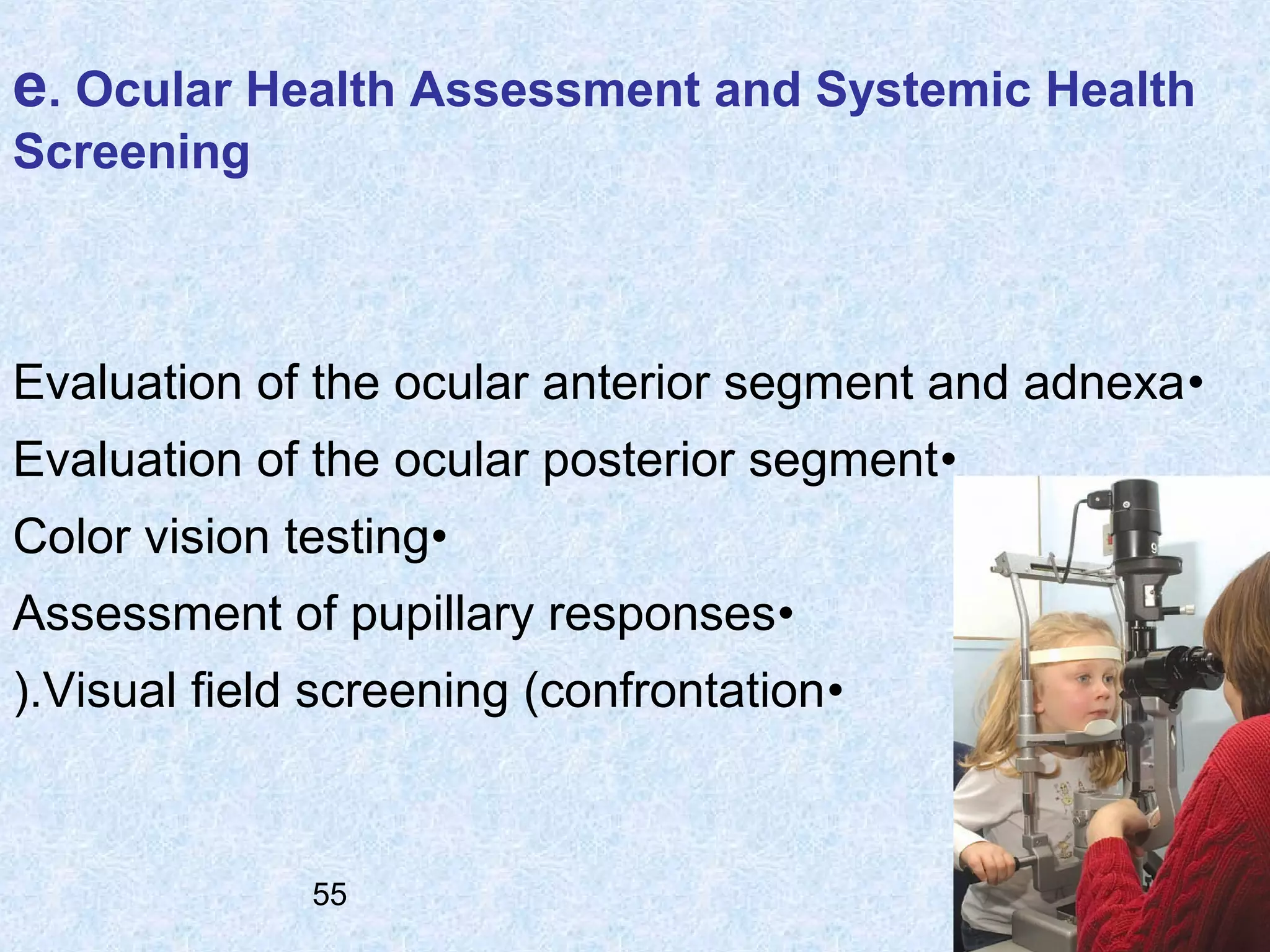
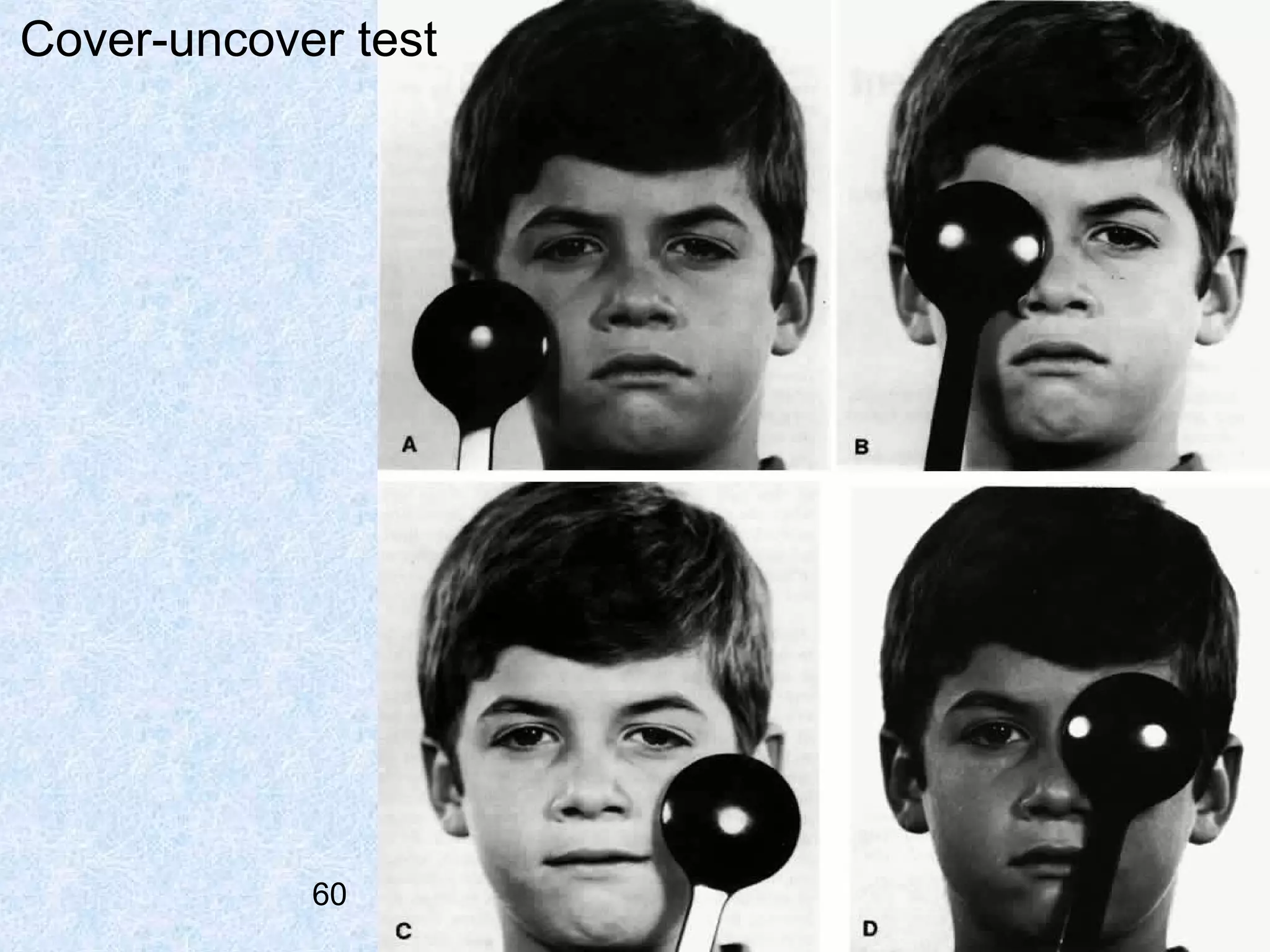
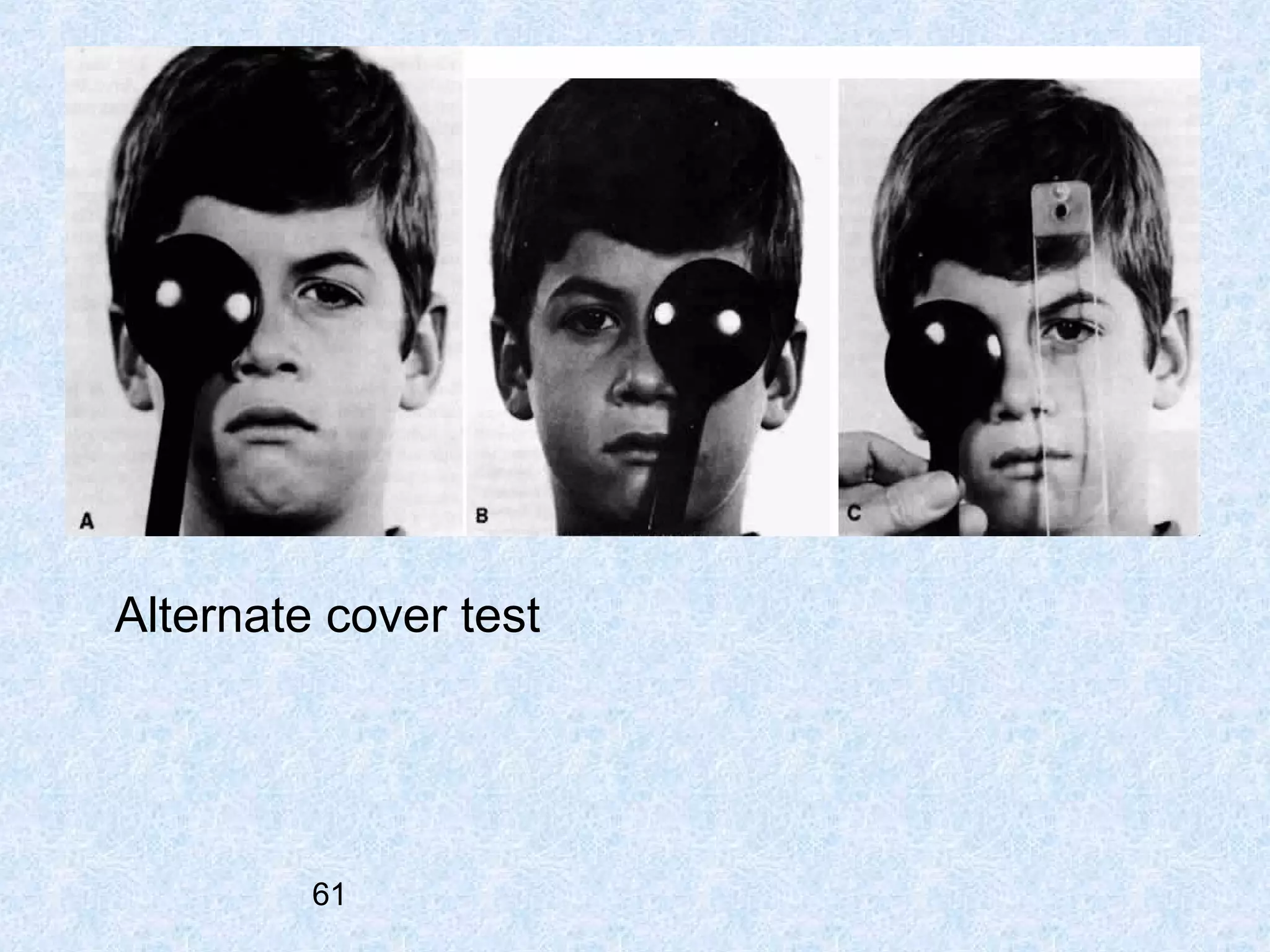
This document provides guidelines for pediatric eye examinations across different age groups. It divides children into infants/toddlers (birth to 2 years 11 months), preschool (3 to 5 years 11 months) and school-age (6 to 18 years). Examination procedures are described for each age group, including visual acuity testing, refraction, binocular vision evaluation, ocular health assessment and more. The document emphasizes using age-appropriate techniques and establishing expected levels of visual function for pediatric patients. Key examination procedures are defined, such as cycloplegic retinoscopy, cover tests, stereopsis tests and others. Recommended examination frequencies are provided based on a patient's age and risk factors.






















































































![OCULAR EMERGENCIES IN PEDIATRICS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ocularemergenciesinpediatricsautosaved-240430020133-f6bf2643-thumbnail.jpg?width=640&height=640&fit=bounds)























