Downloaded 77 times
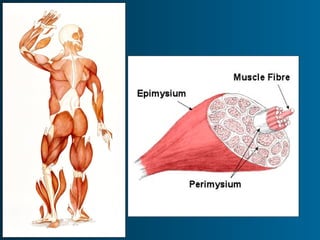
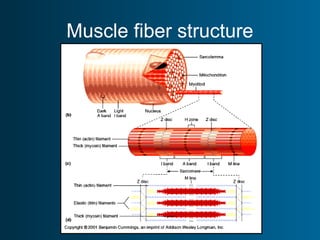
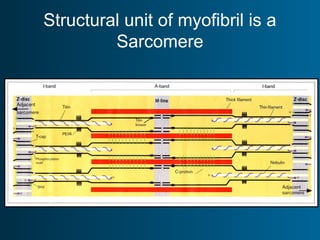
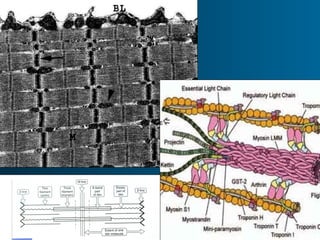
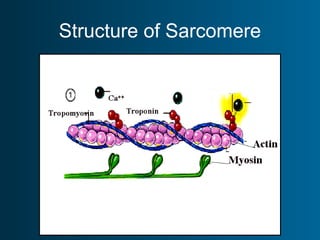
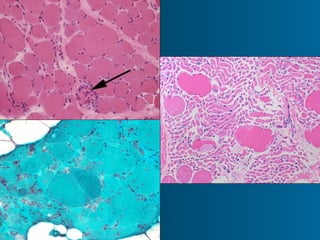
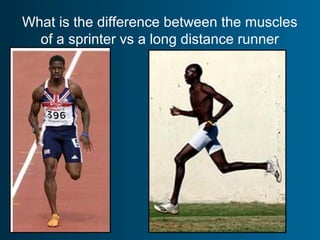
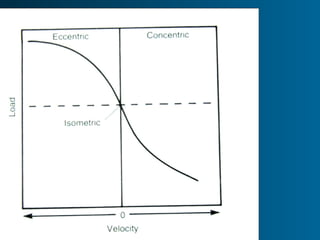
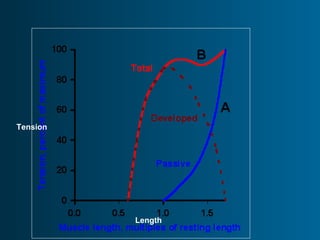
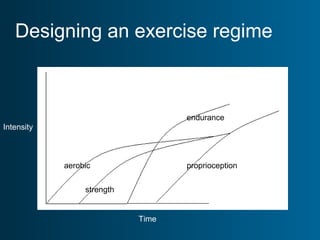
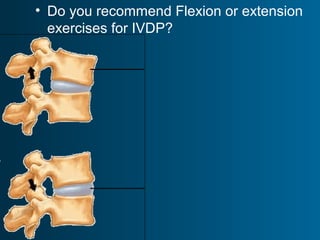



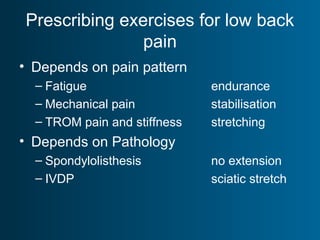
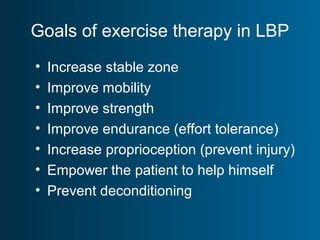



This document discusses muscle structure and function, different types of muscle fibers, and exercise physiology. It provides details on muscle fiber components like myofibrils, sarcomeres, and proteins. It also covers topics like muscle fiber types, contraction types, Frank-Starling law, and therapeutic exercises for conditions like low back pain, shoulder replacement, and ACL reconstruction. The key goals of exercise therapy are to increase mobility, strength, endurance, and proprioception while preventing deconditioning. Exercises must be tailored based on a person's pain pattern and underlying pathology.