Downloaded 70 times


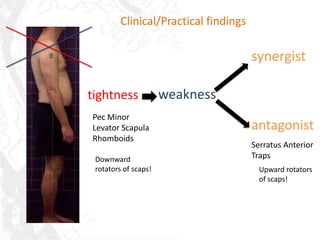
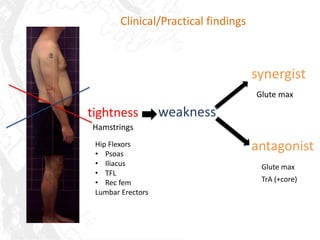

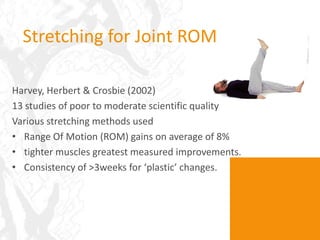
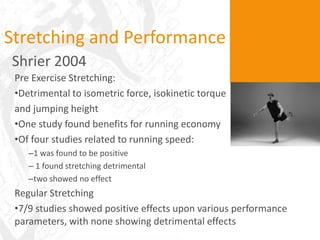







This document discusses flexibility and movement. It explains that tightness can be caused by sedentary lifestyles, injury, poor nutrition, and age. Research shows that stretching provides flexibility gains, especially for tighter muscles, though regular stretching may provide more performance benefits than pre-exercise stretching. Myofascial release techniques like self-massage and foam rolling can improve range of motion and reduce muscle soreness. A comprehensive flexibility program incorporates assessment, exercises to address muscle imbalances, self-myofascial release, stretching, and functional movement training.


























































































