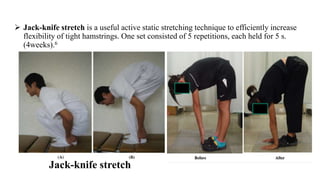
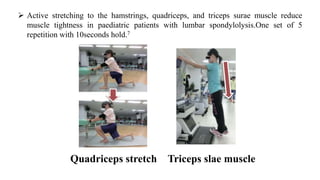
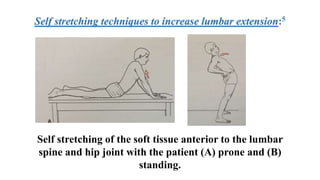
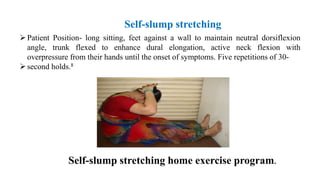
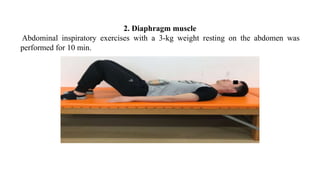
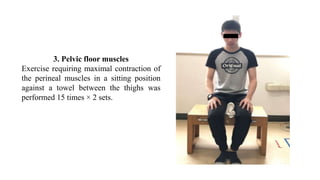
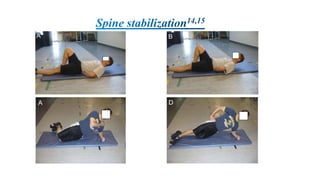
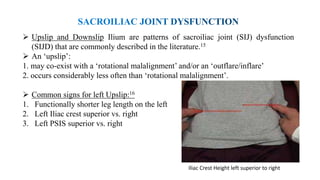
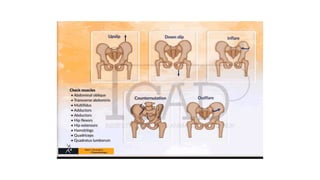
This document discusses various exercises and techniques for rehabilitation of chronic lower back pain (CLBP). It finds that core stability exercises are more effective than stretching alone in improving tonic core muscle strength and endurance for CLBP. Several specific exercises are described to target the transverse abdominis, multifidus, diaphragm and pelvic floor muscles. Stretching techniques for the hamstrings, quadriceps and other muscle groups are also outlined. The document further discusses techniques for addressing sacroiliac joint dysfunction issues like upslips and downslips.