Downloaded 449 times


































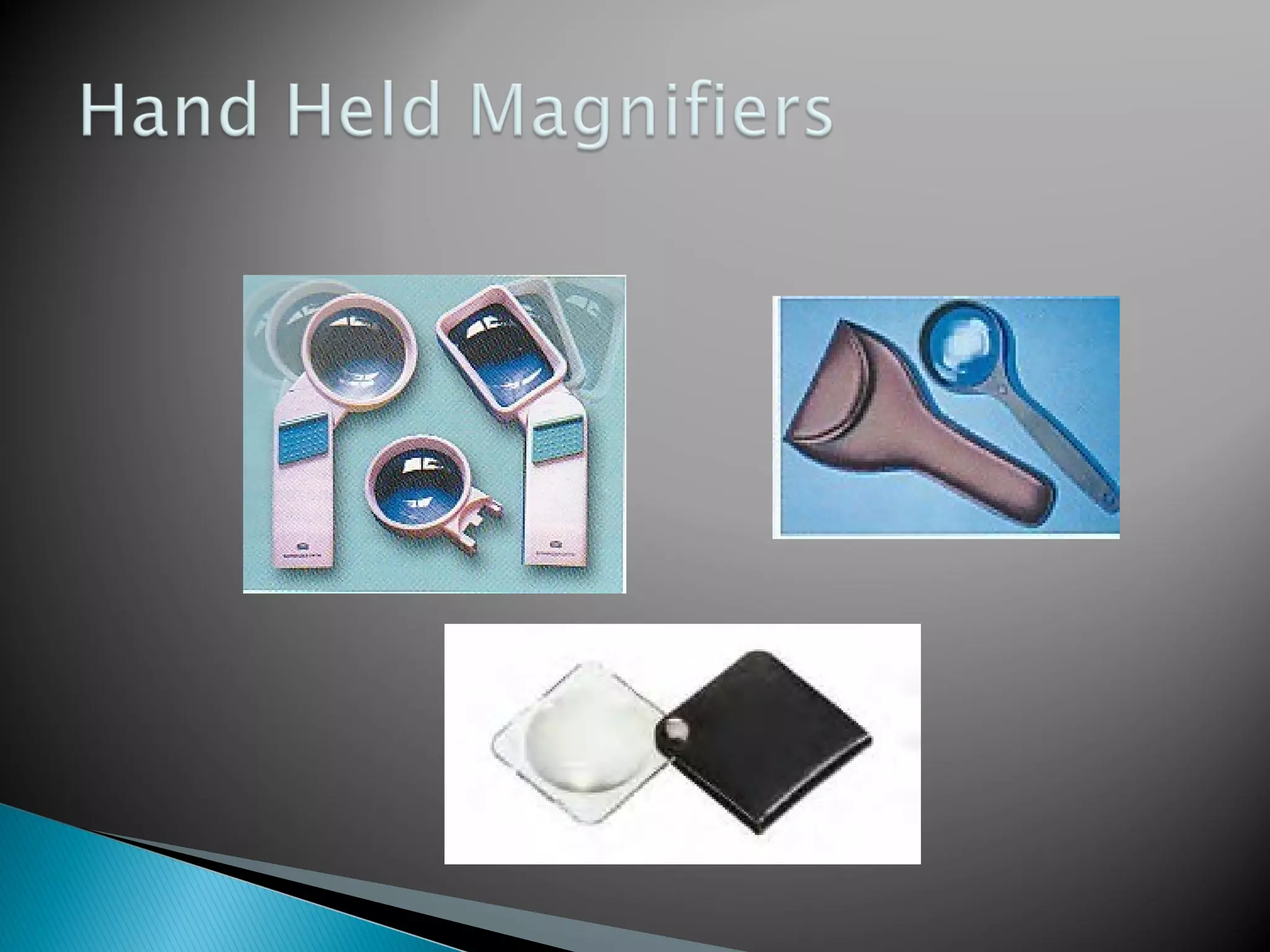













































This document discusses visual disorders and low vision. It defines different levels of visual impairment from moderate to profound based on best corrected visual acuity and visual field diameter. Causes of low vision including various eye diseases are described. Methods of low vision evaluation and different low vision devices like magnifiers, telescopes, electronic devices are explained. Low vision rehabilitation strategies including use of assistive devices and training are also summarized.





















![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)