Dr. Richa Naik describes the process for prescribing spectacles, including:
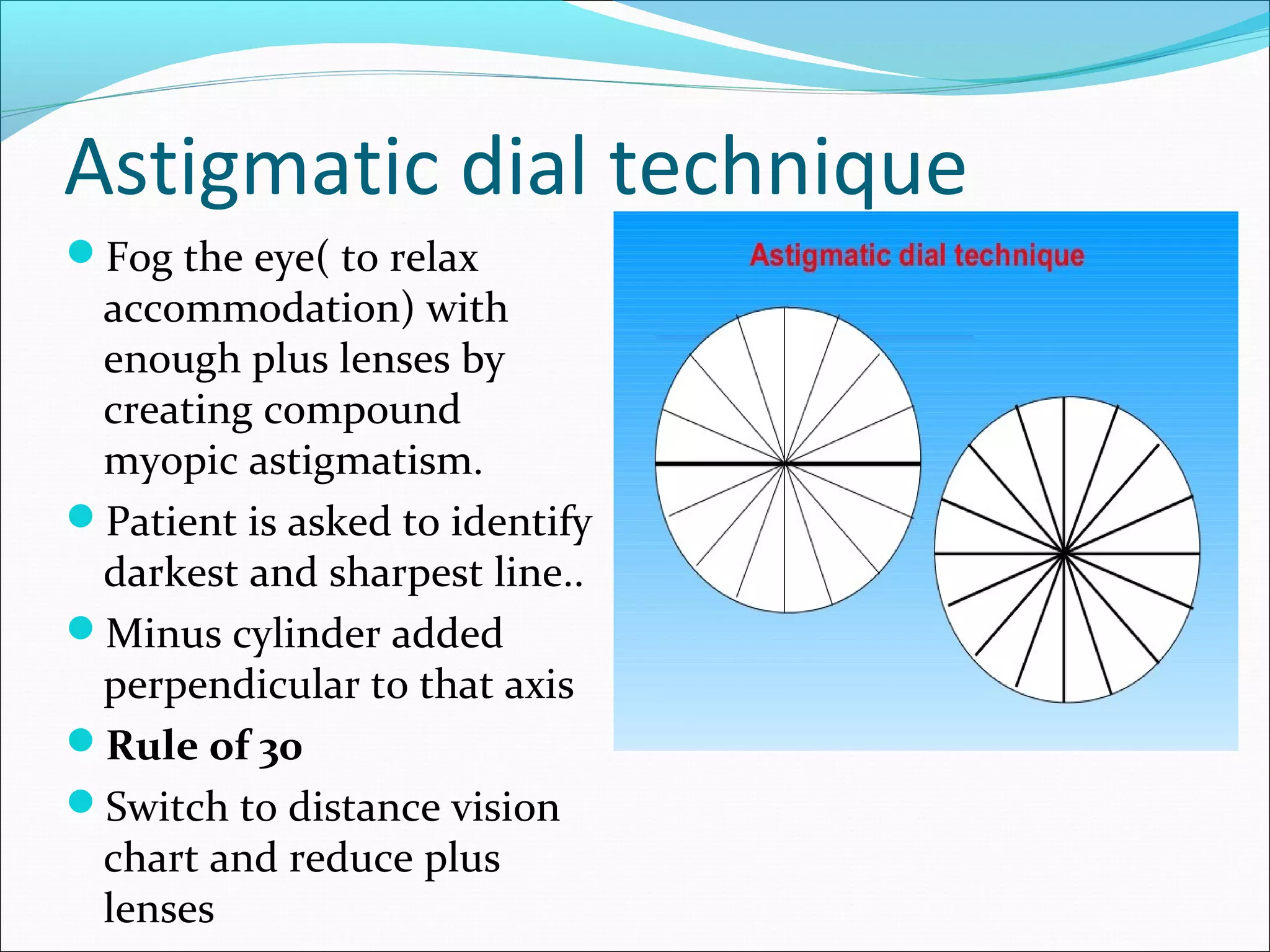
1. Conducting objective and subjective refraction tests to determine the prescription.
2. Providing full correction for most myopia and hyperopia cases, though some require undercorrection.
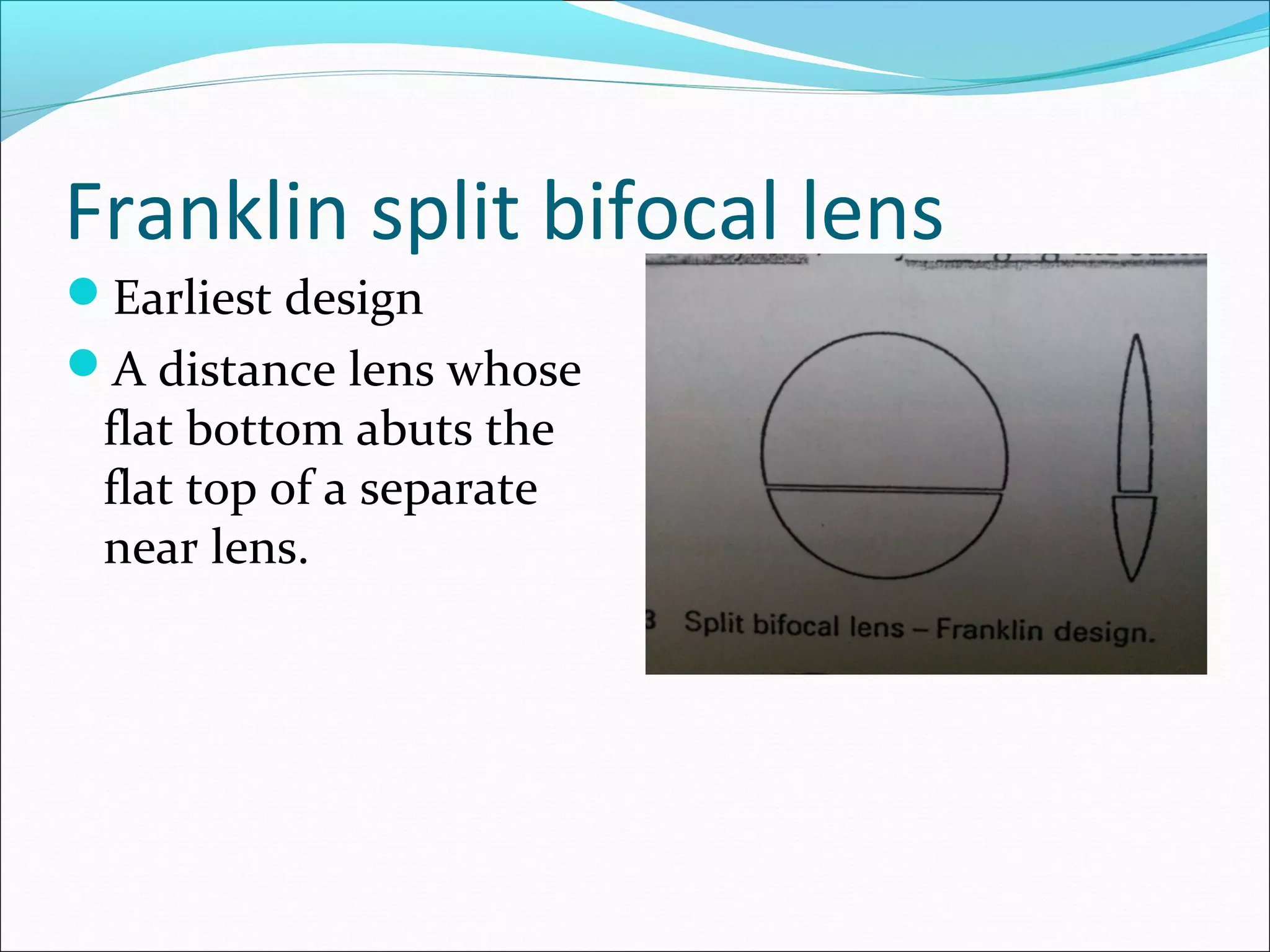
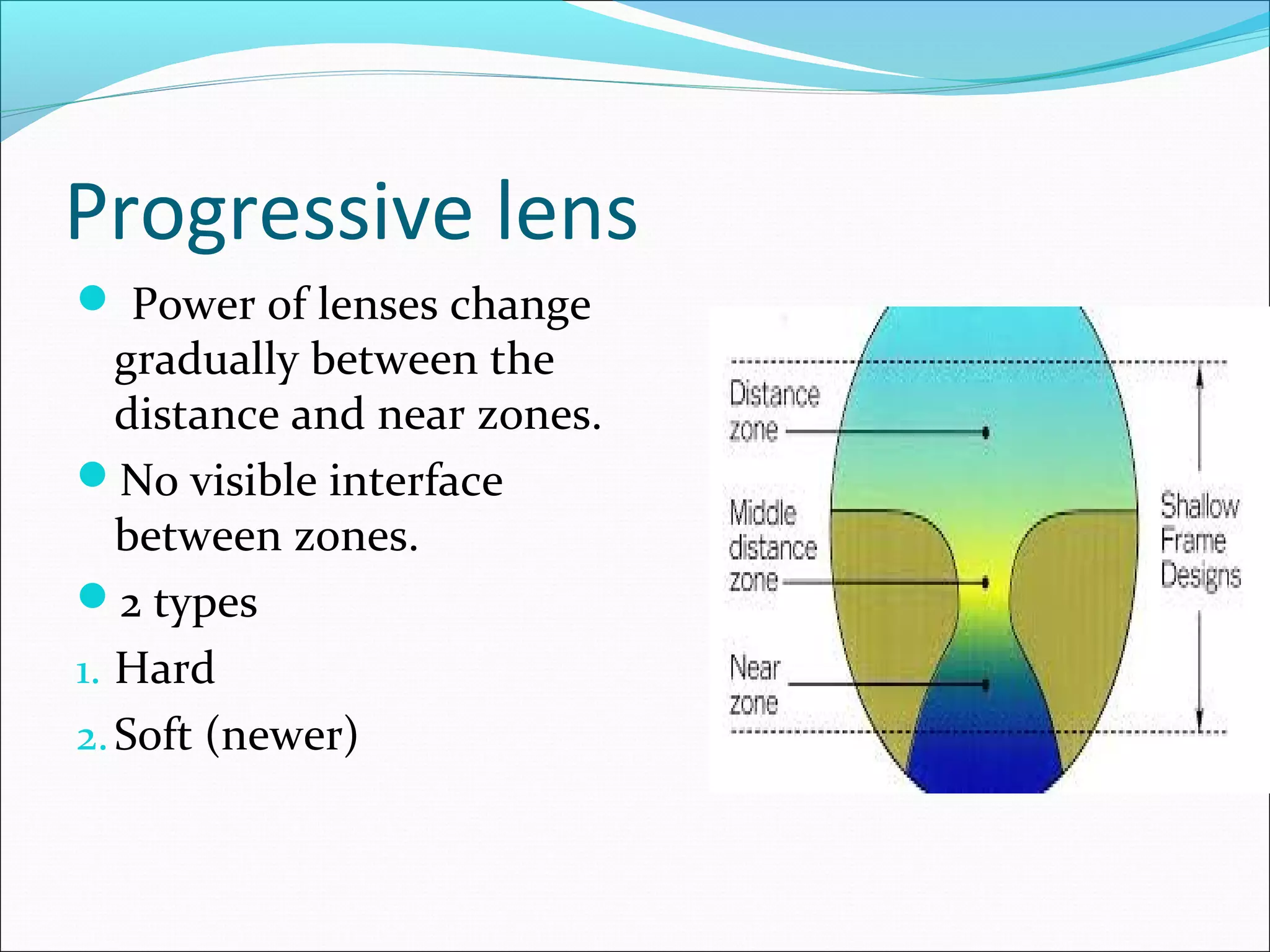
3. Choosing lens types and materials based on the prescription and patient needs, such as polycarbonate lenses for safety or progressive lenses for presbyopia.
4. Adjusting the prescription over time as the patient's vision or needs change.















































![Optics of contact lens and nomenclature copy [repaired] (1)](https://cdn.slidesharecdn.com/ss_thumbnails/opticsofcontactlensandnomenclature-copyrepaired1-170218054900-thumbnail.jpg?width=640&height=640&fit=bounds)










































































