Downloaded 65 times
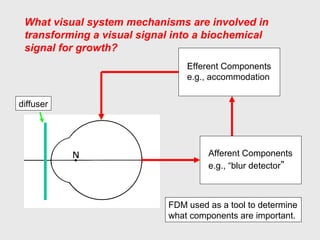
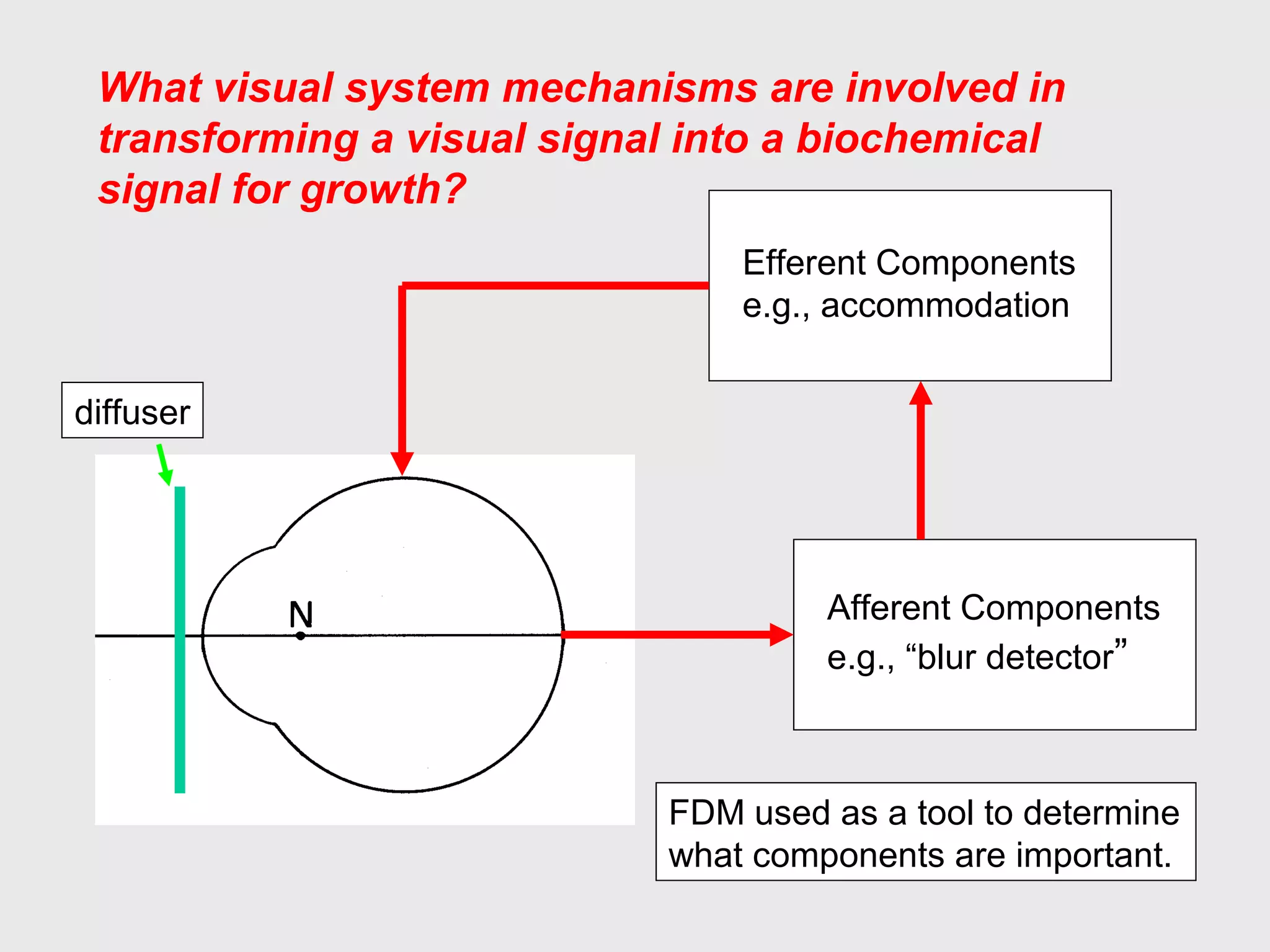
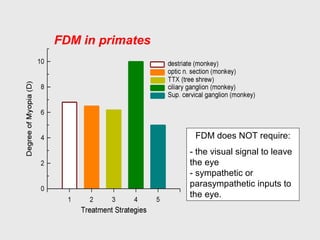
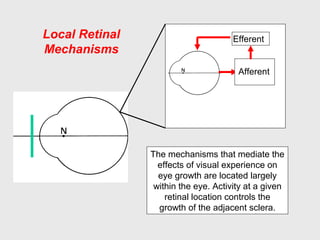
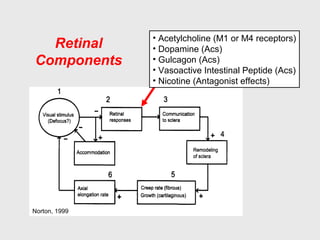
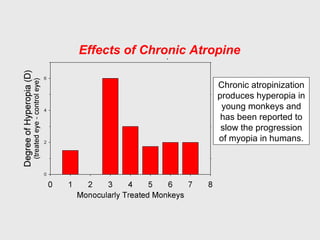
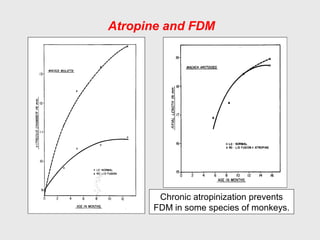
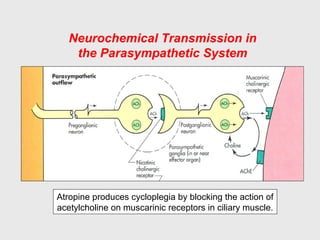
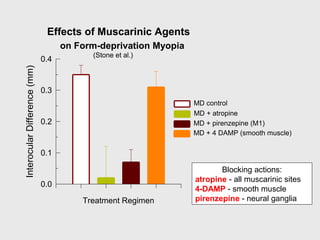
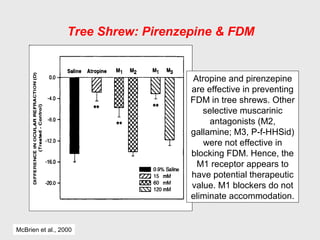
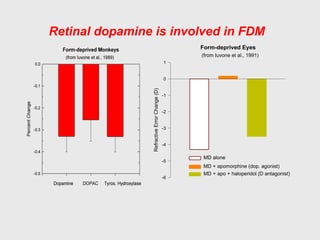
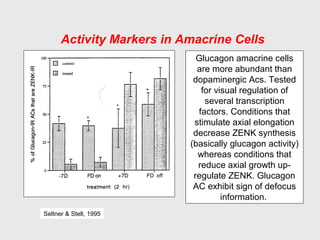
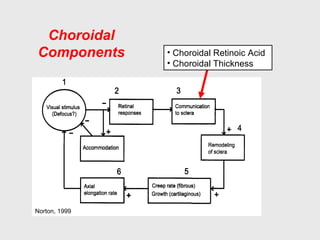
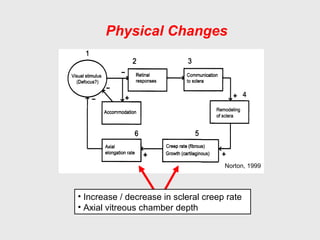

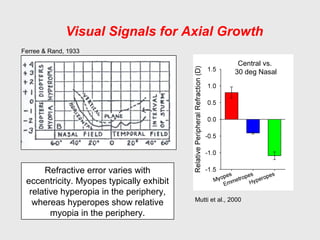

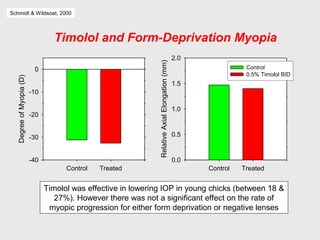
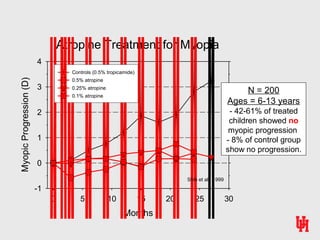

The visual system mechanisms that transform a visual signal into a biochemical signal for eye growth involve both afferent and efferent components located within the eye. Activity at a given retinal location controls the growth of the adjacent sclera. Key retinal components that regulate eye growth include acetylcholine, dopamine, glucagon, and components in the choroid such as retinoic acid. During myopic eye growth, the sclera exhibits increased creep rates and decreased proteoglycan synthesis. Atropine treatment has been shown to significantly reduce the progression of myopia compared to controls.






















































































