Downloaded 43 times

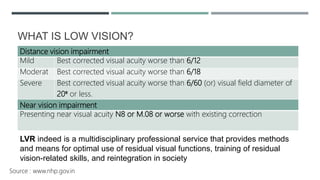
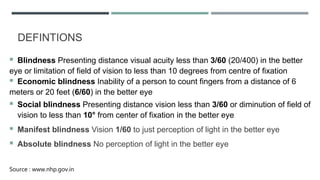
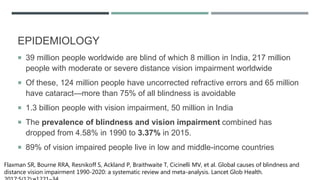
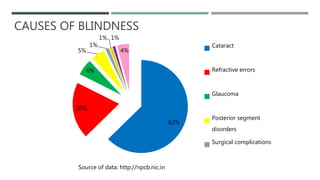
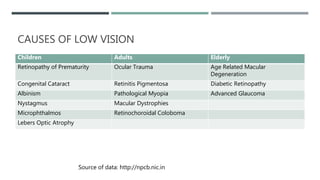
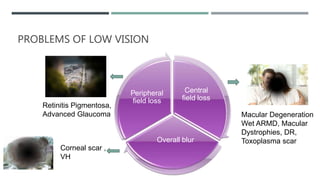
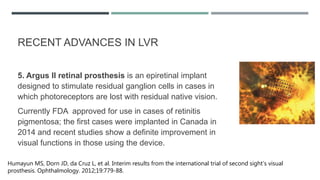
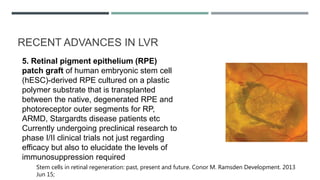
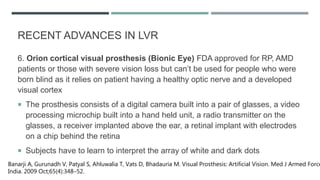

The document discusses low vision rehabilitation, including definitions of low vision, epidemiology of visual impairment, approaches to assessing patients with low vision, types of low vision aids, and recent advances in the field. It provides details on the history and assessments involved in low vision rehabilitation, as well as optical and non-optical devices that can help patients with low vision maximize their remaining vision.



































































