
Downloaded 11 times
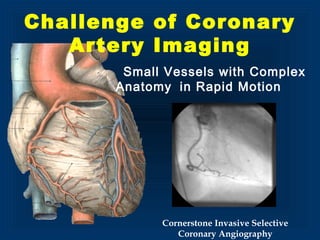
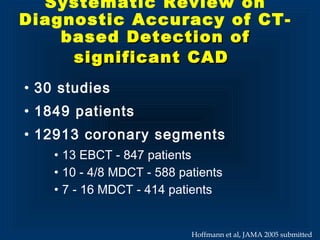
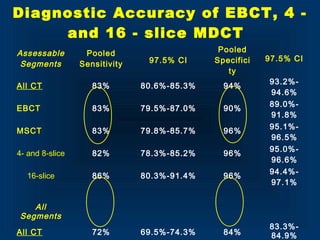
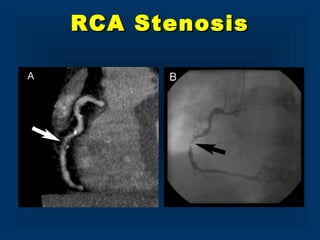
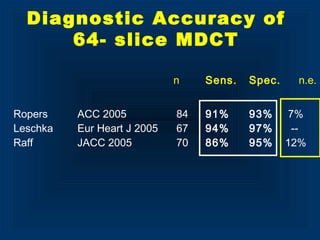
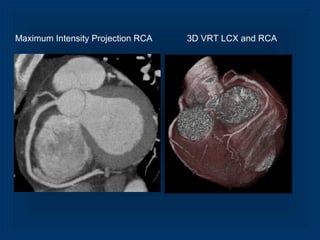
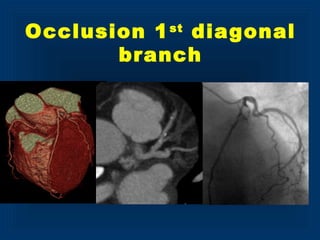
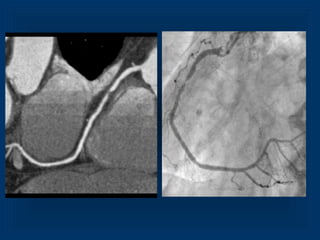

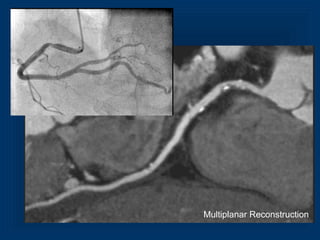
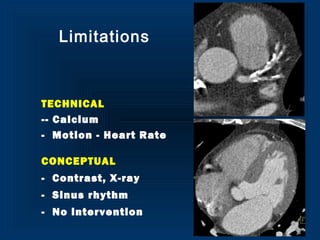
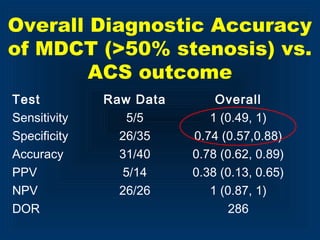
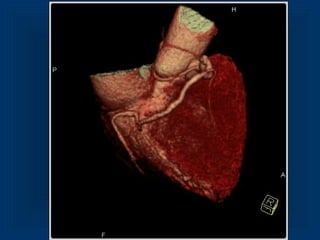
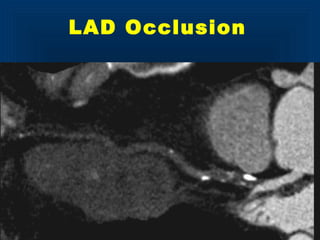
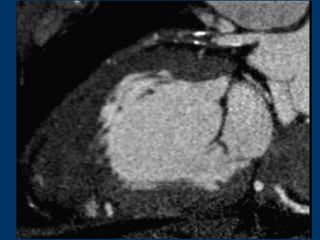

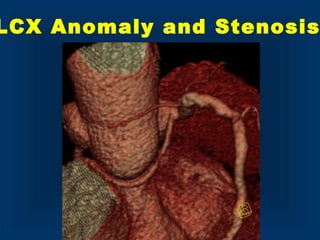
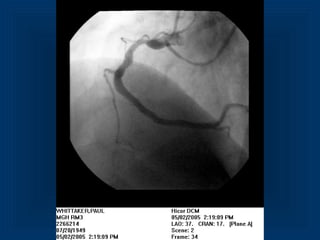


This document summarizes the use of noninvasive MDCT imaging of the coronary arteries. It discusses the challenges of imaging small, rapidly moving coronary vessels. MDCT allows for successful coronary imaging with temporal resolution of 330-400ms, spatial resolution of 0.4-0.75mm, coverage of the heart in a single breath hold of 8-14 seconds. Sensitivity for detecting coronary stenosis is 80-86% for 4-16 slice MDCT and specificity is 90-97%. Potential clinical applications include decreasing invasive angiograms, improving risk assessment, detecting anomalies, and evaluating bypass grafts. Larger clinical trials are still needed to determine the impact on patient management.






































































































