
Download to read offline














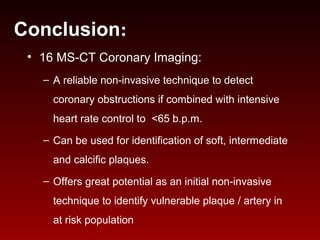

1) Growing evidence suggests that CT-based characterization of coronary plaques and arteries is possible and may serve as an initial screening tool for at-risk patients. 2) 16 slice MS-CT can reliably detect coronary obstructions over 50% if combined with heart rate control under 65 bpm and can identify soft, intermediate, and calcified plaques. 3) Combining CT imaging with serum markers may provide a more powerful predictive value for identifying vulnerable plaque.









































































































