
Download to read offline
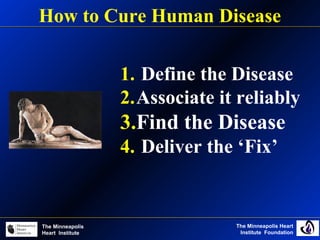


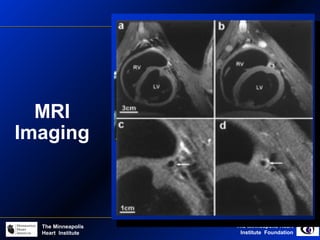
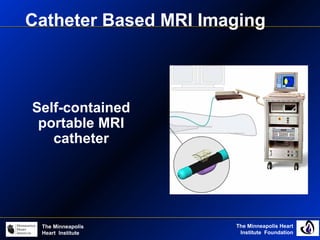
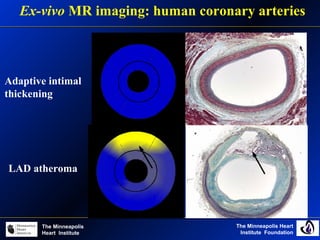

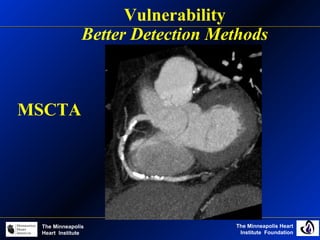
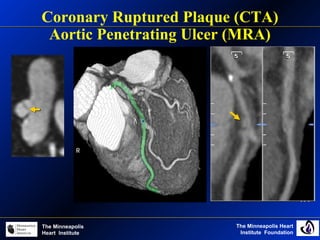
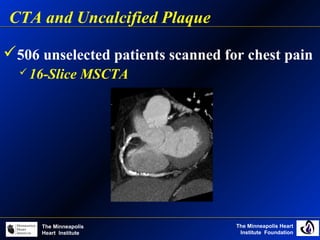
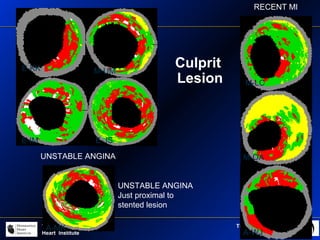
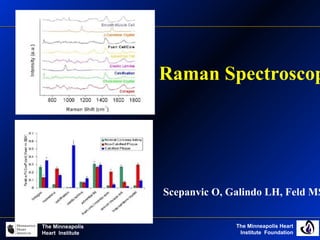
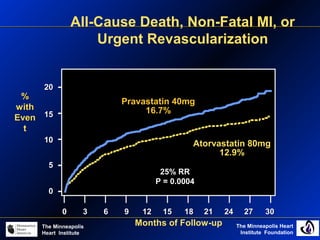
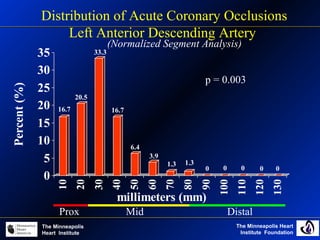
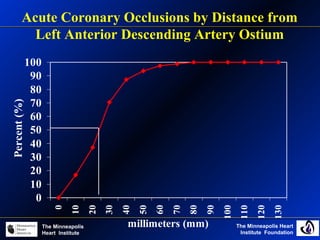
The document discusses vulnerable plaque and challenges in detecting and treating it. It describes various imaging techniques for detecting vulnerable plaque such as thermography, MRI, CT angiography, and optical coherence tomography. However, it notes that while these can identify high-risk features, it remains unclear what exactly defines vulnerable plaque and whether imaging findings truly correlate with risk. The document also notes that while statins reduce events, the relationship between plaque burden and events is unclear, and better defining and detecting the disease is still needed before new therapies can be developed.































































































