
Download to read offline






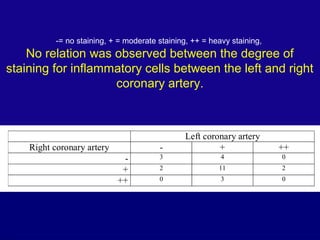

This document summarizes a post-mortem study examining the prevalence of inflammatory cells in non-ruptured atherosclerotic plaques. The study found that moderate or heavy staining for macrophages was present in 45% of femoral artery cross-sections and 84% of femoral arteries had at least one cross-section with moderate/heavy inflammation. There was no observed relationship between the degree of inflammation in the left and right coronary arteries within individuals, indicating the level of local inflammation is locally determined with little predictive value for other arteries.




































































































