Downloaded 704 times
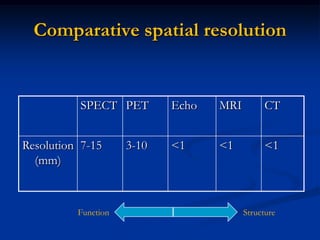
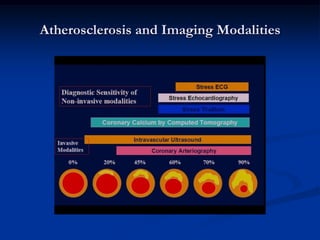
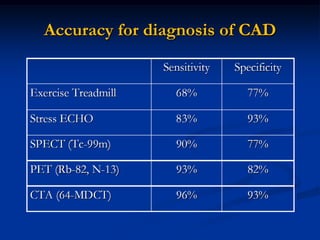
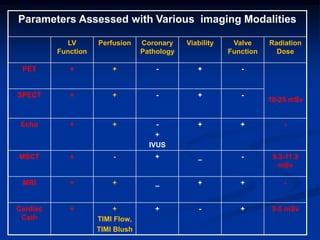

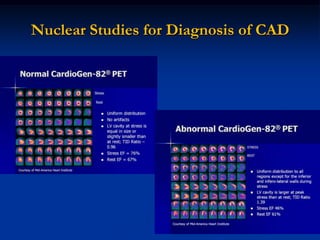
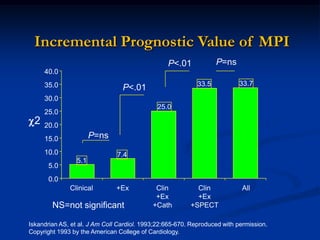
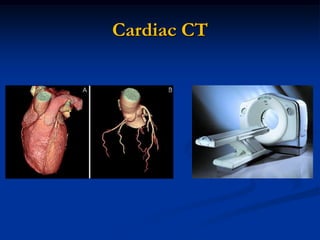
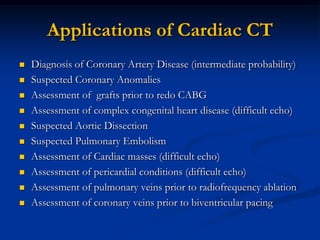
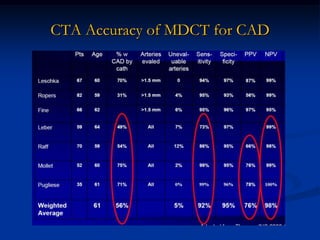
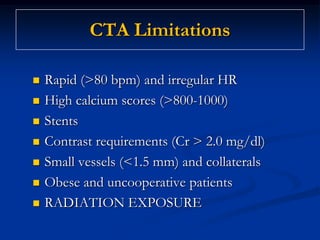
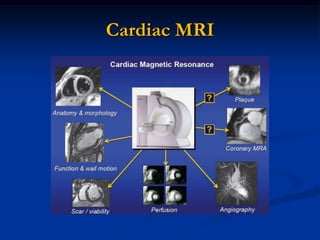
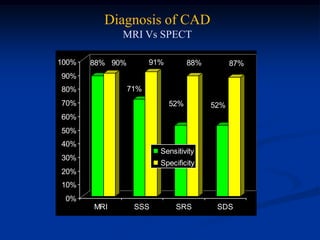
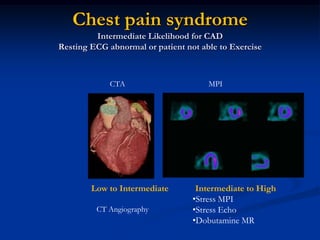
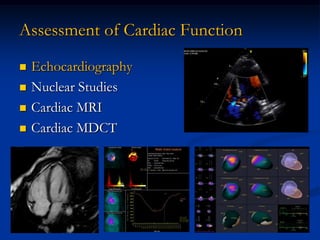
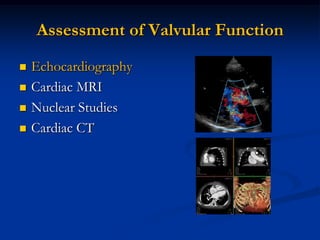
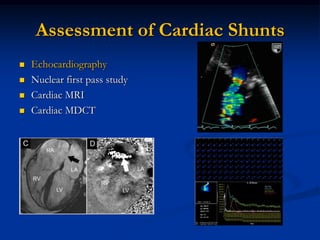
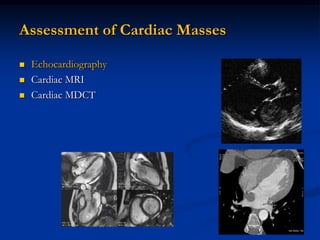
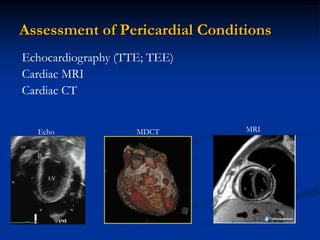
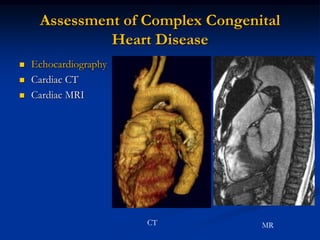
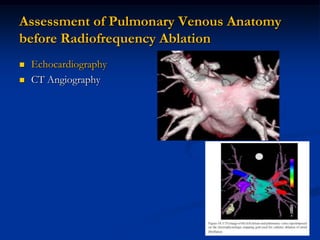
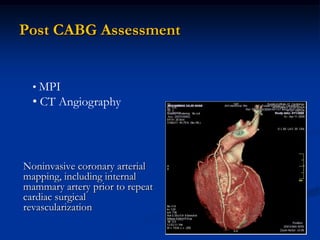
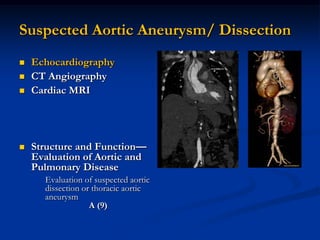
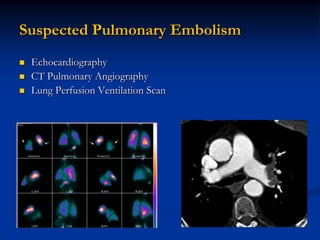
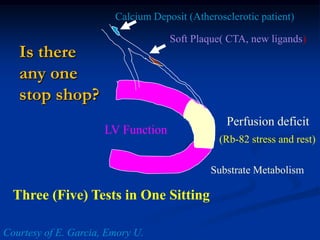


Non-invasive imaging plays an important role in the management of cardiovascular diseases. Different imaging modalities have advantages and limitations. Echocardiography is useful for assessing cardiac structure and function but limited for coronary artery disease evaluation. Nuclear imaging can evaluate perfusion and function but not coronary anatomy directly. CT and MRI can assess coronary anatomy in addition to function but CT involves radiation. The appropriate choice of imaging modality depends on the clinical question and no single test can replace all others for evaluating cardiovascular diseases. Integrating complementary information from different tests provides the most comprehensive assessment.























































