
Download to read offline
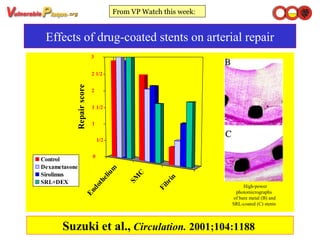
1) Drug-coated stents, particularly those coated with sirolimus, have shown promise in reducing restenosis compared to bare metal stents. Sirolimus inhibits cell proliferation and has been shown in studies to reduce intimal hyperplasia and restenosis in animal models by 50% or more. 2) A study by Suzuki et al. found that a sirolimus-coated stent reduced restenosis by 50% through inhibiting cellular proliferation in a dose-dependent manner compared to a bare metal stent. Adding dexamethasone to the coating did not provide additional benefit. 3) If results of the RAVEL clinical trial showing "zero" restenosis out to 5 years





































































































