Downloaded 534 times

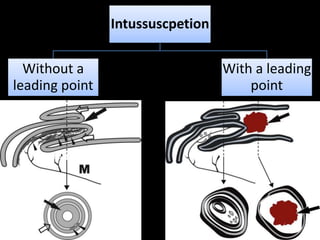
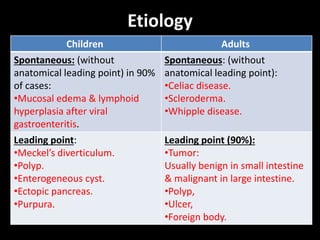
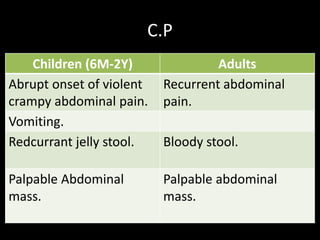
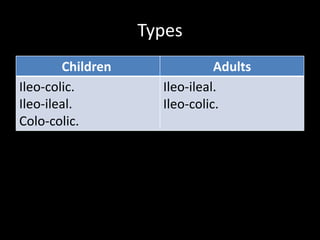


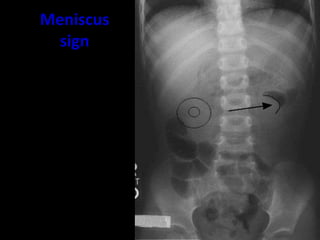

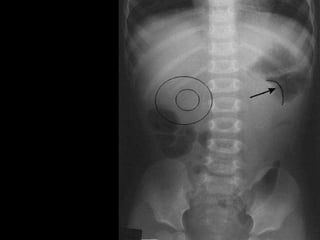

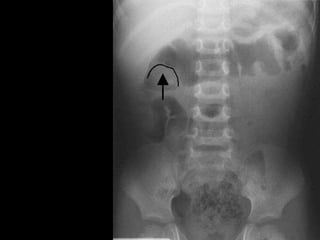
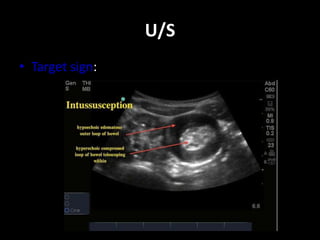

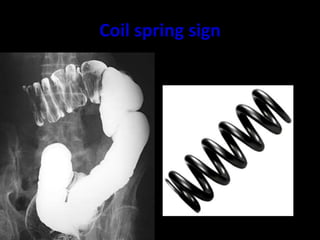

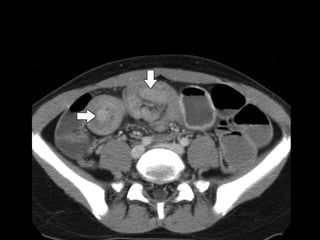
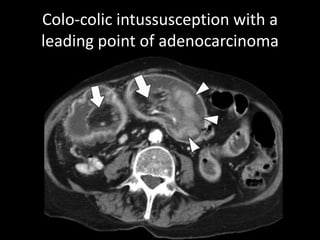
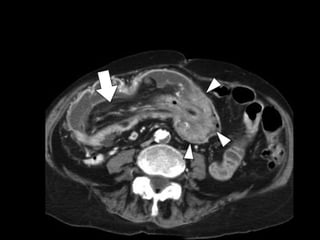

Intussusception is the telescoping of one segment of the intestine into another. It occurs more commonly in children between 6 months and 2 years of age and is often caused by viral gastroenteritis leading to mucosal edema and lymphoid hyperplasia. In adults, intussusception usually has an identifiable anatomical lead point such as a tumor, polyp, ulcer, or Meckel's diverticulum. Symptoms include abdominal pain, vomiting, and bloody stools. Diagnosis can be made using imaging studies like ultrasound, X-ray, or barium enema which may show signs like a target or meniscus.






















































































