Downloaded 450 times





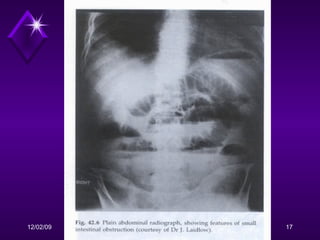







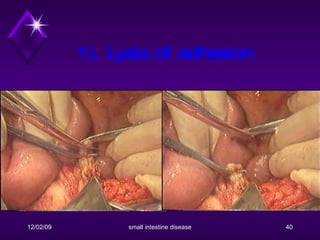







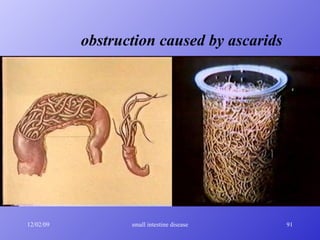
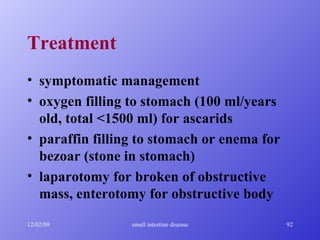















The patient presented with symptoms of intestinal obstruction including abdominal pain, nausea, vomiting and abdominal distension. Physical exam revealed abdominal tenderness and laboratory tests showed signs of dehydration and inflammation. Radiographic imaging confirmed multiple dilated loops of small bowel consistent with mechanical intestinal obstruction. The obstruction was determined to be complete based on symptoms. The patient's history of previous appendectomy suggested the underlying cause was likely adhesive obstruction. Treatment involved fluid resuscitation, gastrointestinal decompression and antibiotics, with potential for surgical lysis of adhesions if symptoms did not improve.























































































