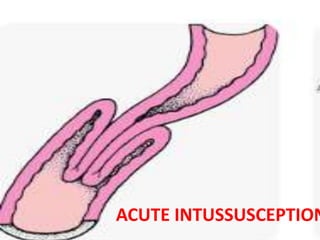
2. When one portion of the
gut invaginates into the
immediately adjacent
loop, the condition is
called intussusception.
3. • Usually proximal loop is invaginated into the
distal bowel.
But rarely the distal loop may invaginate into the
proximal loop and this condition is called
retrograde intussusception (e.g. jejunogastric
intussusception following
gastrojejunostomy).
6. Intussusception is usually acute, but rarely chronic
intussusception may persist for months or years.
Intussusception may recur and this is called recurrent
intussusception.
7. AETIOLOGY
• Broadly speaking there are two varieties of
intussusception —
• I. Where there is definite cause of
intussusception — Secondary intussusception
and
• 2. Where there is no definite cause for
intussusception — Primary or idiopathic
intussusception.
8. 1. SECONDARY INTUSSUSCETION
• Polyp, papilliferous carcinoma, lymphoma, hamartoma,
submucous lipoma, stump of appendix, an inverted
Meckel’s diverticulum etc. may cause intussusception.
• This type of intussusception, which is caused by some
pathology, is known as secondary intussusception.
• This type of intussusception may occur at any age.
• Secondary intussusception usually occurs in the ileum.
• Sometimes intussusception may occur in the early
postoperative period due to inco-ordinale peristalsis in
the small intestine.
9. 2. PRIMARY OR IDIOPATHIC
INTUSSUSCEPTION
• The majority of the intussusceptions belong to
this group.
• This type of intussusception usually occurs in
children between 6 to 9 months of age.
10. PATHOLOGY
• An intussusception is composed of three parts
• (i) the entering or inner tube,
• (ii) the returning or the middle tube
and
• (iii) the sheath or the outer tube.
11. PATHOLOGY
• The entering or inner tube and the returning tube are
together called intussusceptum.
• The ensheathing tube or outer tube is called
intussuscipiens.
• The starting point ofthe intussusception is called the
apex.
• It is the junction of the entering and returning tubes.
• It is the fixed point of intussusception and
intussusception progresses at the cost of the
ensheathing tube or the outer tube.
• The site where the retuning layer and the ensheathing
layer meet is called the neck and this point varies as
the intussusception progresses.
13. • As the intussusception progresses, the mesentery
of the entering and returning tubes is dragged
alongwith the gut through the neck of the
intussusception.
• Gradually the mass of the intussusception by the
pull of the mesentery becomes sausage-shaped
with concavity towards the umbilicus
(approximately the point of attachment of the
mesentery). the mesentery becomes compressed
between the entering and returning tubes.
• In the beginning the mesentery become
constricted and severe venous engorgement and
oedema of the wall of the intussusceptum
oedematous intussusceptum may cause total
intestinal obstruction.
15. PATHOLOGY
• If the mesentery is quite long intussusception can even
present through the rectum at the anal canal pull on
the mesentery becomes sufficient enough to occlude
the arteries.
• This causes onset of gangrene
• Gangrene is dependent upon the tightness of the
invagination and it often occurs in ileocolic
intussusception ileocaecal valve exerts pressure on the
mesentery.
• The returning layer near the apex is the first site to
gangrene.
• Gangrene may cause perforation and ultimately
peritonitis.
• The ensheathing tube is hardly affected.
16. • In rare instances gross adhesion may develop
at the neck between intussusceptum and
intussuscipiens, develops in such case, the
whole mass of intussusceptum becomes
necrosed and sloughs out.
• This brings cure.
18. CLINICAL FEATURES
• Onset is usually sudden. The child screams
with abdominal pain, which is colicky in
nature.
• Alongwith the pain the child draws up his legs.
During the attack the child may vomit.
• But remember that vomiting is a late feature
and usually does not appear before 24 hours
of the onset of the disease.
19. CLINICAL FEATURES
• Such attacks are also accompained by facial
pallor.
• The attacks usually last for a few minutes and
recur every 15 minutes.
• In between the attacks the child lies
motionless and looks very drawn.
• Patient may pass a few normal motions before
current jelly stool is passed.
20. CLINICAL FEATURES
• In long continued and untreated cases pain
becomes continuous. After 2 or 3 days, the
abdomen gradually starts distending.
• Vomiting becomes copious.
• Absolute intestinal obstruction occurs and
death is the ultimate result from intestinal
obstruction alone or peritonitis following
gangrene and perforation
21. PHYSICAL SIGNS
• The abdomen becomes voluntarily contracted
during paroxysms of pain.
• In early cases distension is not noticed.
• Distension only appears after 2 or 3 days of
the commencement of the disease.
• If the abdomen is carefully palpated between
the attacks one may feel a lump under the
right or left costal margin.
22. PHYSICAL SIGNS
• This lump is a sausage-shaped lump with
concavity towards the umbilicus.
• Right iliac fossa is peculiarly empty on palpation.
called Signe-de-Dance.
• This is due to the fact that the If terminal part of
ileum and caecum do not remain m right iliac
fossa, but arc involved in intussusception and arc
tclcscopcd through the ascending colon,
transverse colon and descending colon according
to the various stages.
23. PHYSICAL SIGNS
• RECTAL EXAMINATION should always be
performed One may feel the intussusceptum if
it has reached the rectum.
• It will feel very much like cervix uteri in the
vagina.
• In majority of cases the apex of the
intussusception cannot be felt per rectum but
the finger will be smeared by blood-stained
mucus.
• This will give a definite clue to the diagnosis.
24. PHYSICAL SIGNS
• In very occasional cases intussusception may
actually protrude through the anus when the
patient possesses an unusually long
mesentery.
• In this case it looks like a prolapse.
25. SPECIAL INVESTIGATIONS
• X-ray of the abdomen shows absence of caecal
gas shadow and increased gas shadows in the
small intestine.
• Barium Enema Radiography is very diagnostic
when the intussusception has passed distally
through ileocaecal valve.
• When the intussusception has reached at least
the ascending colon the barium will stop
intussusceptum and there it will show a ‘pincer-
shaped ’ or ‘colied-spring ’ deformity or ‘pitch
fork.
26. • Barium enema has got a therapeutic value, in
the sense that the pressure of the barium
enema may cause spontaneous reduction of
the intussusception.
28. TREATMENT
PREOPERATIVE MANAGEMENT
• Intra- venous fluid administration should be
started immediately and appropriate fluid
resuscitation should be begun.
• Decompression of the small intestine through
nasogastric suction is similarly important.
• Prophylactic antibiotics should be given if
symptoms have been present for more than
24 hours.
29. HYDROSTATIC REDUCTION
When infants present with less than 24 hours of
symptoms. hydrostatic reduction is a
successful treatment in 60 to 70% of patients
Barium enema can be used for hydrostatic
reduction of intussusception.
OPERATIVE TREATMENT
RESECTION