Learning Objectives
• 1.Define intussusception and its clinical significance.
• 2. Understand the functional anatomy of the bowel and
how it predisposes to intussusception.
• 3. Explain the pathophysiology and pathogenesis.
• 4. Recognize clinical presentation and diagnostic tools.
• 5. Compare non-surgical vs. surgical management.
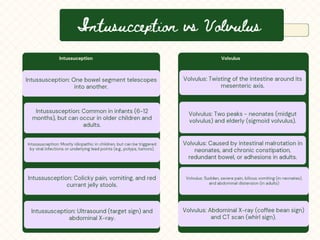
• 6. Differentiate intussusception from volvulus.
3.
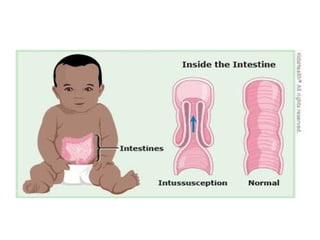
What Is Intussusception?
•• Definition: Telescoping of a proximal bowel
segment (intussusceptum) into a distal
segment (intussuscipiens).
• • Clinical Impact:
• - Leading cause of intestinal obstruction in
infants (6–12 months).
• - Untreated can lead to ischemia, necrosis,
perforation.
5.
Functional Anatomy ofthe Bowel
• • Layers: Mucosa, submucosa, muscularis
propria, serosa.
• • Blood Supply: Superior mesentric artery and
inferior mesenteric artery critical for
perfusion.
• • Innervation: Enteric Nervous System
(Auerbach’s and Meissner’s plexuses).
• • Peristalsis: Coordinated propulsion of
luminal contents.
6.
Pathogenesis
• Pediatric:
• •Idiopathic (80–90%):
• Viral infections eg rota virus and adeno virus lead to
lymphoid hyperplasia (Peyer’s patches) which form a lead
point that anchors and drags the ileum into the cecum
• • Common at ileocecal junction.
• Adult:
• •causes: Tumors, polyps, adhesions,Meckel’s
diverticulum.
7.
Pathophysiology
• 1. Leadpoint formation leading to telescoping.
• 2. Mechanical obstruction leading to colicky
pain/vomiting.
• 3. Venous congestion leading to edema and
red'currant jelly stools.'
• 4. Arterial insufficiency leading to necrosis and
perforation.
Diagnosis
• 1Clinical Diagnosis
•Based on history and physical exam findings:
• Classic triad (colicky pain, vomiting, currant
jelly stools).
• Palpable sausage-shaped mass in the right
upper quadrant (RUQ).
• Lethargy or irritability, especially in infants.
10.
Diagnosis
• Imaging Studies
•Ultrasound (Best Initial Test)
• Shows the classic “target sign” or “doughnut sign”
(layers of telescoped bowel).
• High sensitivity and specificity.
• Abdominal X-ray
• May show air-fluid levels (suggesting obstruction).
• May indicate absence of gas in the RLQ (“Dance
sign”).
• 3. LaboratoryTests (Supportive)
• FBC – May show leukocytosis
(infection/inflammation).
• Electrolytes – To assess dehydration from
vomiting.
13.
Management Algorithm
• •Stable Patient: Air/contrast enema reduction
(80–90% success).
• • Unstable Patient or Failed Enema: Surgery
(manual reduction or resection).
14.
Treatment
• Immediate IVfluid resuscitation to correct fluid
losses and restore fluid, electrolyte and acid base
balance
• Antibiotics to cover for translocation
• NG tube for transfer with IV fluid maintenance and
replacement of NG losses
• Reduction is only attempted once fluid balance is
restored
• Analgesia and sedation may aid process of reduction
15.
Non-Surgical Reduction
• •Procedure: Fluoroscopic/ultrasound-guided
air enema.
• • Contraindications: Peritonitis, perforation,
prolonged symptoms.
• • Success Rate: 80–90% in early cases.

































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







