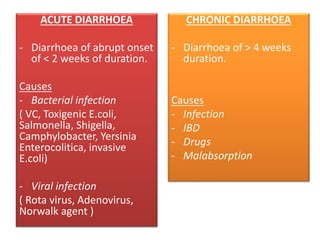
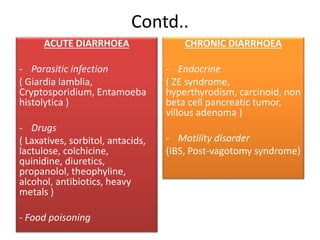
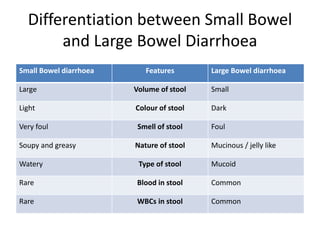
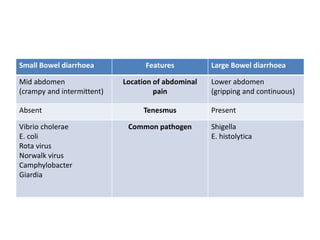
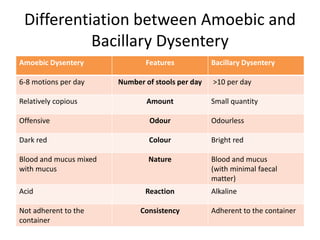
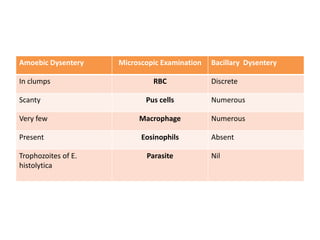
The document provides a comprehensive overview of diarrhoea, including its definition, mechanisms, types (acute and chronic), clinical classification, and differentiation between small and large bowel diarrhoea. It details causes, assessment methods, laboratory investigations, and treatment options, such as rehydration and specific antibiotics based on the pathogen. Additionally, it explains the differentiation between amoebic and bacillary dysentery and the clinical implications of diarrhoea in HIV patients.