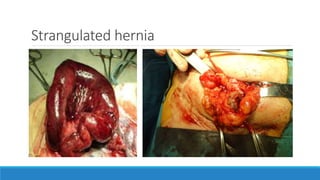
Strangulated inguinal hernias occur when herniated tissue becomes trapped within the hernia sac, cutting off blood flow. This can lead to tissue death. Symptoms include swelling, pain, and signs of bowel obstruction. Diagnosis is usually made through surgical exploration, which may involve bowel resection. While tension-free mesh repairs have been successfully used in strangulated hernias, non-mesh techniques are generally preferred due to the risk of mesh infection in contaminated fields. Proper surgical technique and mesh choice can help reduce infection risks for tension-free repairs in strangulated hernias.