Downloaded 858 times






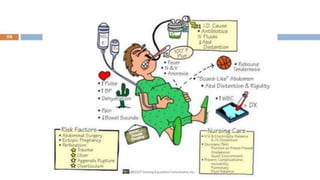
















Intestinal perforation can be caused by factors such as penetrating injuries, blunt trauma, infections, and pre-existing conditions. Diagnosis involves medical history, physical examination, and various imaging techniques, with treatment primarily surgical to repair the perforation and address underlying causes. Post-operative care and monitoring for complications are critical for patient recovery.

















































































