Downloaded 303 times


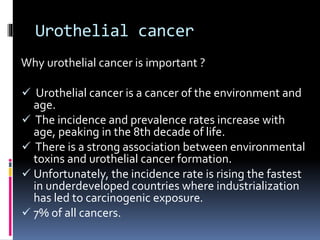
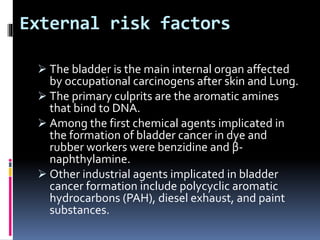


![Postoperataive adjuvant intravesical chemotherapy
for non-muscle invasive bladder cancer[1, 2] :
One postoperative intravesical dose (within 24h,
but usually immediately after resection) has
been shown to reduce recurrence, but not
progression, of disease
Mitomycin 40 mg in 20 mL sterile water or
Epirubicin 80 mg in 40 mL sterile water or
Thiotepa 30 mg in 15 mL sterile water or
Doxorubicin 50 mg in 20 mL sterile water](https://image.slidesharecdn.com/neoplasmofbladder-140919084141-phpapp01/85/Neoplasm-of-bladder-47-320.jpg)
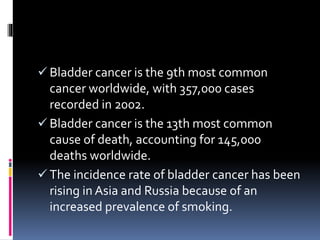
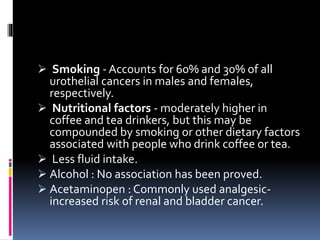
![High grade or T1 disease:
Management of T1 tumors with TURBT is generally
not adequate enough; use of intravesical bacillus
Calmette-Guerin (BCG) after TURBT is
recommended
Intravesical adjuvant immunotherapy for non-muscle
invasive bladder cancer[1, 3, 2] :
BCG 81 mg (TheraCys) or 50 mg (TICE BCG) in 50
mL sterile saline instilled into the bladder through a
catheter and held for 2h; it is instilled into the
bladder weekly for 6wk
Maintenance therapy: 81 mg intravesically given on
Days 1, 8, and 15 of Months 3, 6, 12, 18, 24, and 36
after initiation](https://image.slidesharecdn.com/neoplasmofbladder-140919084141-phpapp01/85/Neoplasm-of-bladder-48-320.jpg)


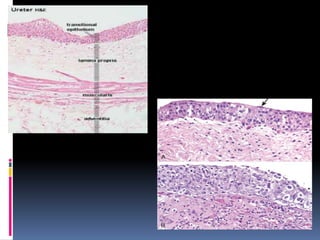
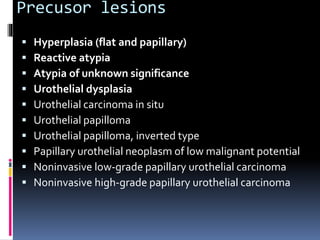
The document discusses the anatomy and histology of the bladder and various benign and malignant tumors that can occur. It provides details on: 1. The anatomy of the bladder including its shape, surfaces and location in the pelvis. 2. The normal histology of the bladder wall and urothelial lining. 3. Various benign tumors of the bladder including epithelial metaplasia, leukoplakia, inverted papilloma, nephrogenic adenoma, leiomyoma, cystitis cystica and glandularis. 4. Risk factors, pathology, clinical features and staging of urothelial cancer of the bladder, which represents the majority of bladder cancers.





























![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Bladder Cancer NMIBC [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/non-muscleinvasivebladdertumoredmond-140716212950-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























































