Downloaded 1,660 times




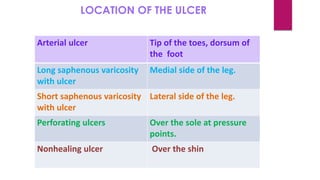
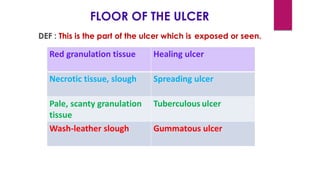
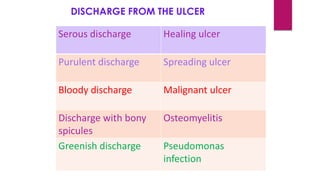
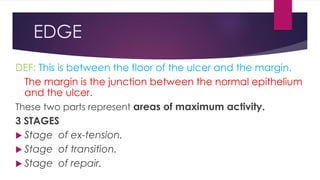
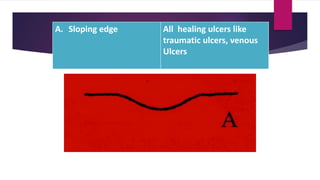
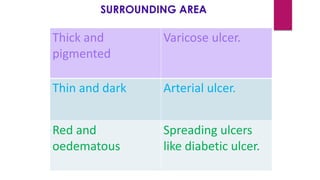

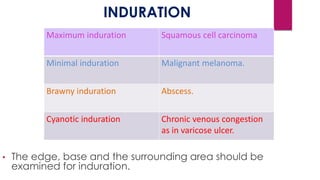




The document outlines the definition, etiology, grading, and classification of ulcers as well as various types including arterial, venous, tropical, and diabetic ulcers. It discusses their examination, including inspection and palpation, along with the characteristics of edges, discharge, and surrounding areas. Management involves addressing underlying causes, conducting investigations, and employing various treatment methods such as debridement, dressings, and potential skin grafting for chronic ulcers.






























































































