Downloaded 973 times
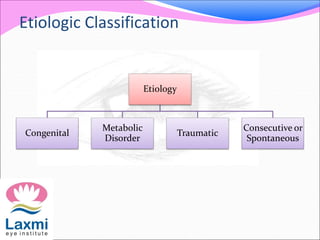
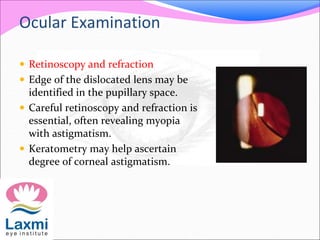
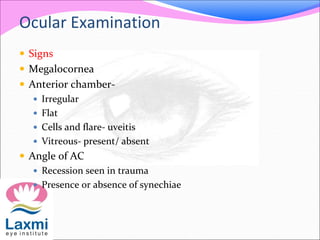
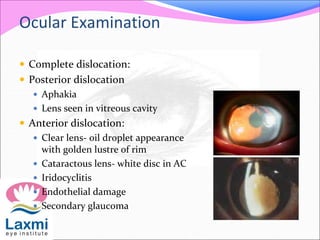
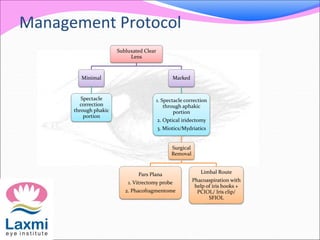
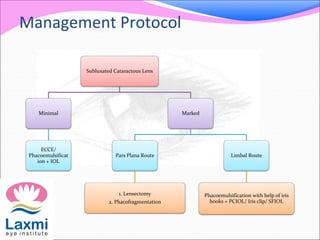
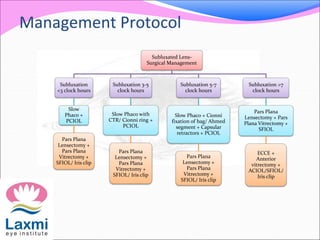
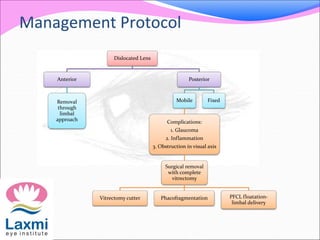



This document provides information about ectopia lentis, or displacement of the crystalline lens. It begins with classifications of ectopia lentis based on location and etiology. Congenital causes like Marfan syndrome and homocystinuria are described. Presentation, examination findings, complications, workup, and management approaches are outlined. Surgical techniques depend on degree and location of lens subluxation/dislocation and may involve lens removal with or without intraocular lens implantation. Management of subluxated lenses in children poses additional challenges due to risk of complications with contact lenses or suture-fixated intraocular lenses.











































































































