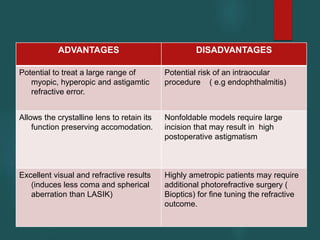
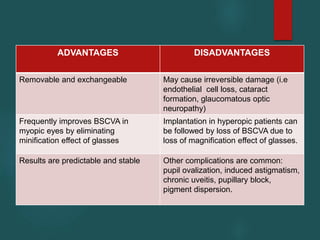
Phakic intraocular lenses (IOLs) are artificial lenses designed to correct moderate to high refractive errors while preserving the natural crystalline lens, making them a suitable option for patients with severe myopia and hyperopia. They have several advantages over traditional laser procedures, such as maintaining corneal structure, predictable results, and rapid visual recovery, although they also carry risks like intraocular complications. The document outlines the history, various types of phakic IOLs, surgical procedures, and potential complications associated with their implantation.