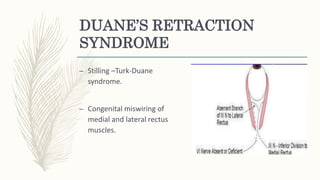
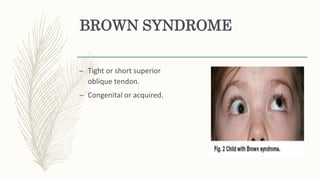
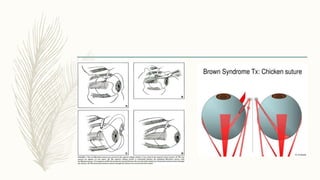
This document discusses restrictive strabismus, which is characterized by limited eye movement out of proportion to the ocular deviation. It can be caused by mechanical or neurological issues. The document then classifies restrictive strabismus as either congenital (e.g. Duane's retraction syndrome, Brown's syndrome) or acquired (e.g. thyroid ophthalmopathy, orbital injury, tumors). Specific conditions like Duane's retraction syndrome and Brown's syndrome are further described in terms of symptoms, prevalence, and management approaches including non-surgical and surgical options.



































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)







