1. DUANE’S RETRACTIONSYNDROME
The syndrome in its classic form is characterized by the following features:
• Limitation of abduction and/or adduction
• Retraction of globe on adduction
• Narrowing of palpebral fissure on adduction and widening on abduction.
• Frequently, upshoot or downshoot of eye on attempted adduction.
3.
ETIOLOGY
Currently, itis believed that Duane's syndrome is a congenital cranial
dysinnervation disorder (CCDD) of brainstem origin rather than occurring
due to structural anomalies of the muscles.
Probable cause of dysinnervation is: Embryopathy and Heriditary
Paradoxical innervation of the horizontal rectus muscles is the main
etiological factor.
4.
Paradoxical innervationis there for both LR and MR rectus muscles, so both
co-contract during abduction and adduction resulting in:
• Abduction—limitation
• Adduction—limitation
• Palpebral aperture—narrowing in primary position as well as in
adduction and abduction.
• Globe retraction
5.
Classification of Duane'ssyndrome
Huber classified Duane's syndrome into three types I, II, III and recently
type IV has also been added.
Clinical feature
Clinical features of Duane's syndrome can be discussed as:
(I) General features,
(II) Features related to ocular motility defect,
(III) Associated ocular abnormalities, and
(IV) Associated systemic abnormalities.
6.
I. General features
•Females are more frequently involved than males.
• Left eye is more commonly affected (75%) than the right.
• Bilateral involvement is less frequent (20%) than unilateral occurrence.
7.
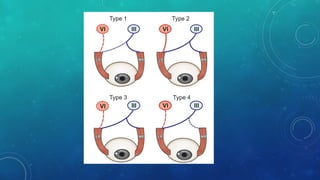
Characteristic features oftype I DRS are:
In primary position eye may be orthophoric, esotropic (more common) or
exotropic.
On attempted abduction since LR muscle does not receive innervation, so
• Abduction is limited markedly,
• Palpebral fissure is normal or slightly widened, and
• Globe is slightly protused. This happens as a result of relaxation of both LR
and MR muscles during abduction.
9.
On attempted adduction,since along with MR, LR also gets anomalous
innervation, so due to contraction of MR and LR:
• Adduction is present but limited, due to co contraction of MR and LR
• Palpebral fissure becomes narrow, and
• Globe is retracted,
• Upshoot or downshoot of the globe may occur due to slippage caused by
co-contraction of MR and LR.
10.
Characteristic features oftype II DRS are:
In primary position, eyeball may be orthophoric, esotropic or exotropic (more
common).
On attempted abduction
• Abduction is normal or there may be slight limitation due to subnormal
innervation and/ or associated MR contracture.
• Palpebral aperture remains normal or slightly widens
11.
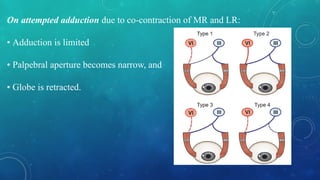
On attempted adductiondue to co-contraction of MR and LR:
• Adduction is limited
• Palpebral aperture becomes narrow, and
• Globe is retracted.
12.
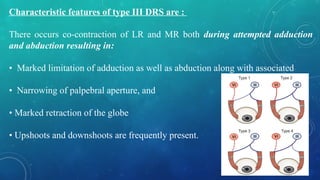
Characteristic features oftype III DRS are :
There occurs co-contraction of LR and MR both during attempted adduction
and abduction resulting in:
• Marked limitation of adduction as well as abduction along with associated
• Narrowing of palpebral aperture, and
• Marked retraction of the globe
• Upshoots and downshoots are frequently present.
13.
Characteristic features ofType IV Duane syndrome include:
• Exotropia in primary gaze,
• Face turn opposite the involved eye,
• Essentially full abduction of the involved eye,
• Absent adduction of involved eye with simultaneous abduction in gaze opposite
the involved eye, and
• Narrowing of the palpebral fissure.
Associated ocular abnormalities
•Anisometropia with hyperopia
• Other ocular abnormalities include optic nerve hypoplasia, morning glory
syndrome, congenital ptosis, nystagmoid movements, congenital cataract,
heterochromia iridis, persistent hyaloid arteries, choroidal colobomas,
districhiasis, pupillary anomalies, keratoconus, microphthalmos and many
others
16.
Associated systemic abnormalities
Klipple-Feilsyndrome, Goldenhar's syndrome, facial hemi atrophy, cervical
spina bifida, umbilical hernia, polydactly, Chiari I malformations, sensori neural
hearing deficits and Wildervank syndrome or cervico-oculoacoustic syndrome
(combination of Duane's syndrome, sensori neural hearing loss and Klippel-Fiel
anomaly of the spine).
17.
DIAGNOSIS
• Duane's retractionsyndrome is usually diagnosed on version tests by its typical
signs.
MANAGEMENT
1. Non-surgical measures Refractive error and/ or amblyopia, when present,
should be treated first.
2. Management of Eso-DRS:
MR recession of affected eye, Assymetric bilateral MR recession
3. Management of Exo- DRS :
LR recession, LR recession Y Split
4. Management of ortho DRS : orthotropic in primary position but there is
severe globe retraction with upshoots and downshoots.
Symmetrical recession of MR and LR of the affected eye
19.
2. BROWN SYNDROME
Brownsyndrome refers to mechanical restriction (a significant limitation) of
elevation in adduction caused by an overly taut superior oblique tendon of the
same eye.
Etiology
• The condition may be congenital or acquired.
• Originally, Brown divided the syndrome into True sheath syndrome (now
congenital) and Simulated sheath syndrome (now acquired).
20.
Congenital Brown'ssyndrome is presently thought to be caused by a
congenitally taut superior oblique tendon (short and inelastic tendon).
Brown thought that these cases occur due to congenitally shortened anterior
sheath of the superior oblique tendon.
This theory has not been proved by subsequent workers.
Parks observed that the superior oblique tendon sheath does not exist at all
and that the term 'superior oblique tendon sheath syndrome' introduced by
Brown is a misnomer.
21.
Acquired Brown's syndromeis presently thought to be caused by an acquired
taut superior oblique tendon, secondary to following conditions:
Tenosynovitis of the superior oblique trochlear apparatus.
Trauma to the trochlear region The 'canine tooth syndrome' of Knapp also falls
into this category.
Surgical trauma has emerged as another cause of acquired Brown's syndrome
(traumatic Brown's syndrome).
Association with other autoimmune diseases like SLE (systemic lupus
erythematosus),Sjögren syndrome and Graves' ophthalmopathy is also
reported.
Idiopathic
22.
CLINICAL FEATURES
Congenitalcases are constant and unilateral in 90% percent of patients.
Most acquired cases are intermittent and more likely to improve
spontaneously
The syndrome is rarely seen in adults.
The clinical features of this syndrome can be divided into main consistent
features and less important variable features.
23.
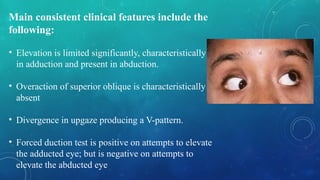
Main consistent clinicalfeatures include the
following:
• Elevation is limited significantly, characteristically
in adduction and present in abduction.
• Overaction of superior oblique is characteristically
absent
• Divergence in upgaze producing a V-pattern.
• Forced duction test is positive on attempts to elevate
the adducted eye; but is negative on attempts to
elevate the abducted eye
24.
Less important andvariable clinical features include:
• Downshoot in adduction.
• Widening of the palpebral fissure on adduction.
• Straight eyes in primary position are present in most patients but a few may
have hypotropia.
• Chin up may be present in patients with hypotropia.
• An audible click may be produced when patients elevate their adducted eye.
Some observers have used the term 'superior oblique click syndrome’.
25.
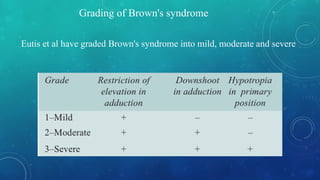
Grading of Brown'ssyndrome
Eutis et al have graded Brown's syndrome into mild, moderate and severe
26.
Differential Diagnosis
1. Inferioroblique paralysis versus Brown's syndrome
• Limitation to elevation in adduction is greater on testing for ductions than
versions in inferior oblique paralysis, while in Brown's syndrome, it is equal.
• Overaction of the superior oblique muscle is typically absent in Brown's
syndrome, while it is present in inferior oblique palsy.
• Forced duction test is positive in Brown's syndrome, while it is negative in
inferior oblique palsy.
• Park's 3-step test is positive in inferior oblique palsy.
27.
2. Other conditionswith restriction of elevation which need to be differentiated
from the Brown's syndrome are double elevator palsy, fracture of the orbital
floor, Graves' ophthalmopathy and congenital fibrosis of the inferior rectus
muscle.
In all these conditions, elevation is equally restricted in adduction, primary
gaze and in abduction;
While in Brown's syndrome, elevation is restricted only in adduction.
28.
MANAGEMENT
1. Acquired casesshould be observed, since spontaneous improvement has
been reported.
Range of eye motility exercises (elevation and adduction exercises)
Steroids either orally or by injection near the trochlea in inflammatory cases.
Correction of the underlying cause, when possible such as trauma to the
trochlea.
2. Surgical treatment. Results of the surgery for this entity are controversial and,
therefore, surgery should only be undertaken in severe (grade 3) cases of
Brown's syndrome (Superior oblique tenetomy, superior oblique tenectomy).
29.
3. MOBIUS SYNDROME
Mobiussyndrome refers to congenital bilateral abducent paralysis associated
with congenital facial palsy with variable other associations.
Etiology and genetics
Mobius syndrome is being considered a heterogeneous group of congenital
disorders caused by developmental defects related to a variety of insults such
as ischaemia, toxic effects of prenatal used drugs such as misoprostol,
benzodiazepines.
30.
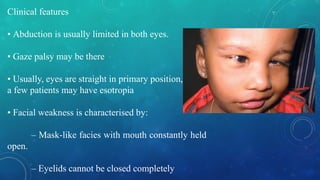
Clinical features
• Abductionis usually limited in both eyes.
• Gaze palsy may be there
• Usually, eyes are straight in primary position,
a few patients may have esotropia
• Facial weakness is characterised by:
– Mask-like facies with mouth constantly held
open.
– Eyelids cannot be closed completely
31.
Associations include:
1. Paralysisor hypoplasia of tongue due to involvement of hypoglossal nerve
with speech and swallowing difficulties are extremely common.
2. Other cranial nerves which can be involved are 3rd, 4th, 9th, and 10th.
3. Craniofacial anomalies which may be associated are epicanthal folds,
microstomia, micrognathia and external ear defects.
4. Limb's abnormalities include webbed fingers and toes, supernumerary digits,
club foot and syndactyly.
5. Deafness and mental retardation are also reported.
32.
6. Congenital heartdefects such a ventricular septal defect are also reported
7. Respiratory defects with tachypnoea and other respiratory difficulties occur in
some patients
MANAGEMENT
• Prevention of exposure keratitis due to facial weakness may be done by
tarsorrhaphy.
• Esotropic patients, though rare, may be managed by MR recessions with or
without LR resection
33.
4. NYSTAGMUS BLOCKAGESYNDROME
The term 'nystagmus blockage syndrome' has been suggested for the
occurrence of esotropia in a child with congenital nystagmus.
It has been reported that in a bid to dampen the nystagmus, there occurs
adduction or excessive convergence which results in esotropia.
34.
CLINICAL FEATURES
1. Esotropia: Characterized in its acute form by an esotropia of early onset with
a variable angle, changing from orthotropia with manifest nystagmus during
periods of visual inattention to esotropia without nystagmus during visual
attention.
2. Nystagmus intensity is inversely proportional to the angle of deviation.
3. Visual acuity is increased with adduction due to dampening of nystagmus.
Therefore, best visual acuity is at near fixation.
4. Pseudoparalysis of both lateral recti results due to maintaining the eyes in a
position of convergence.
35.
5. ADHERENCE SYNDROME
Two types of adherence syndrome, the lateral adherence syndrome and
superior adherence syndrome, have been reported to occur due to
developmental abnormal fascial connections.
In the lateral adherence syndrome, an abnormal fascial connection is seen
between the muscle capsule of the lateral rectus and inferior oblique, which
produces limitation of ocular rotation in the field of lateral rectus muscle.
In the superior adherence syndrome, an abnormal fascial connection exists
between the superior rectus and tendon of the superior oblique, causing
limitation of rotation in the field of superior rectus muscle.
36.
Treatment consistsof severing of all the adhesions after disinsertion of the
lateral or superior rectus muscle.