Downloaded 171 times

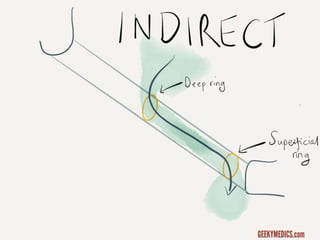
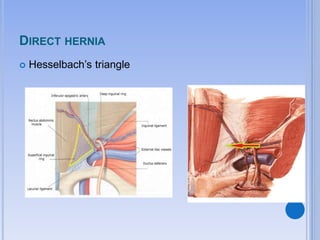
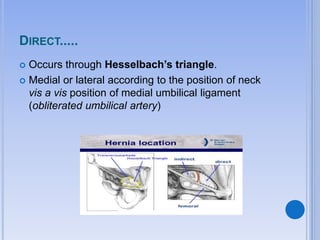
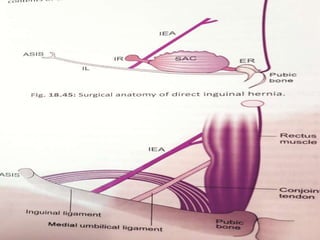

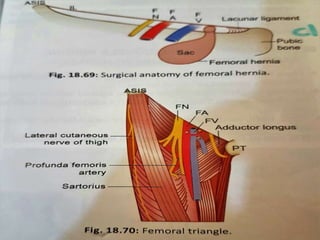
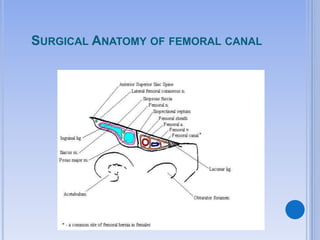
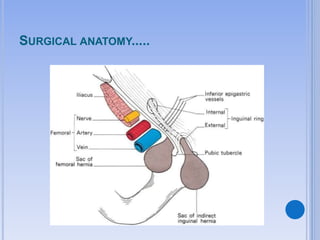
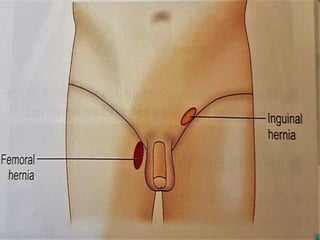
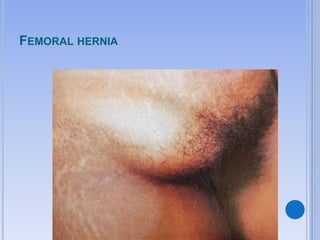
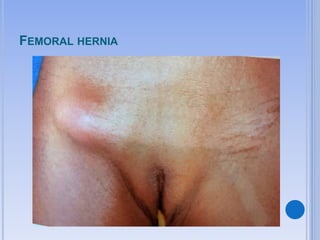


Indirect inguinal hernias are the most common type of groin hernia, accounting for 65% of cases. They occur when the hernia sac passes through the deep inguinal ring to the superficial ring. Direct inguinal hernias are less common, accounting for 10-15% of cases, and occur through Hesselbach's triangle due to weakness in the posterior wall of the inguinal canal. Femoral hernias are more common in females and occur when abdominal contents descend into the femoral canal below the inguinal ligament. Complications of hernias include strangulation, obstruction, and incarceration, while complications of hernia surgery include injury to surrounding nerves and vessels,




























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














