Downloaded 940 times

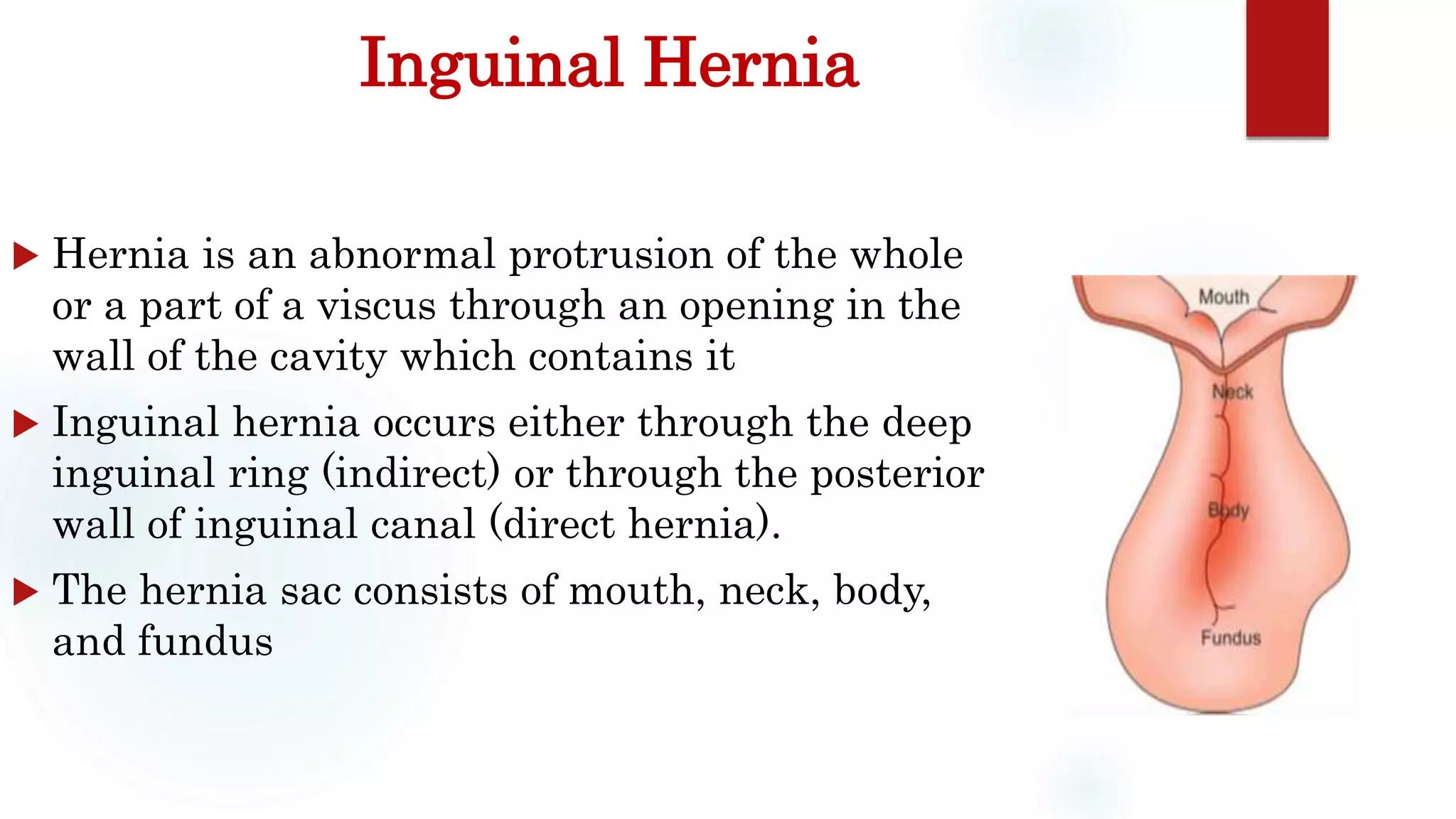










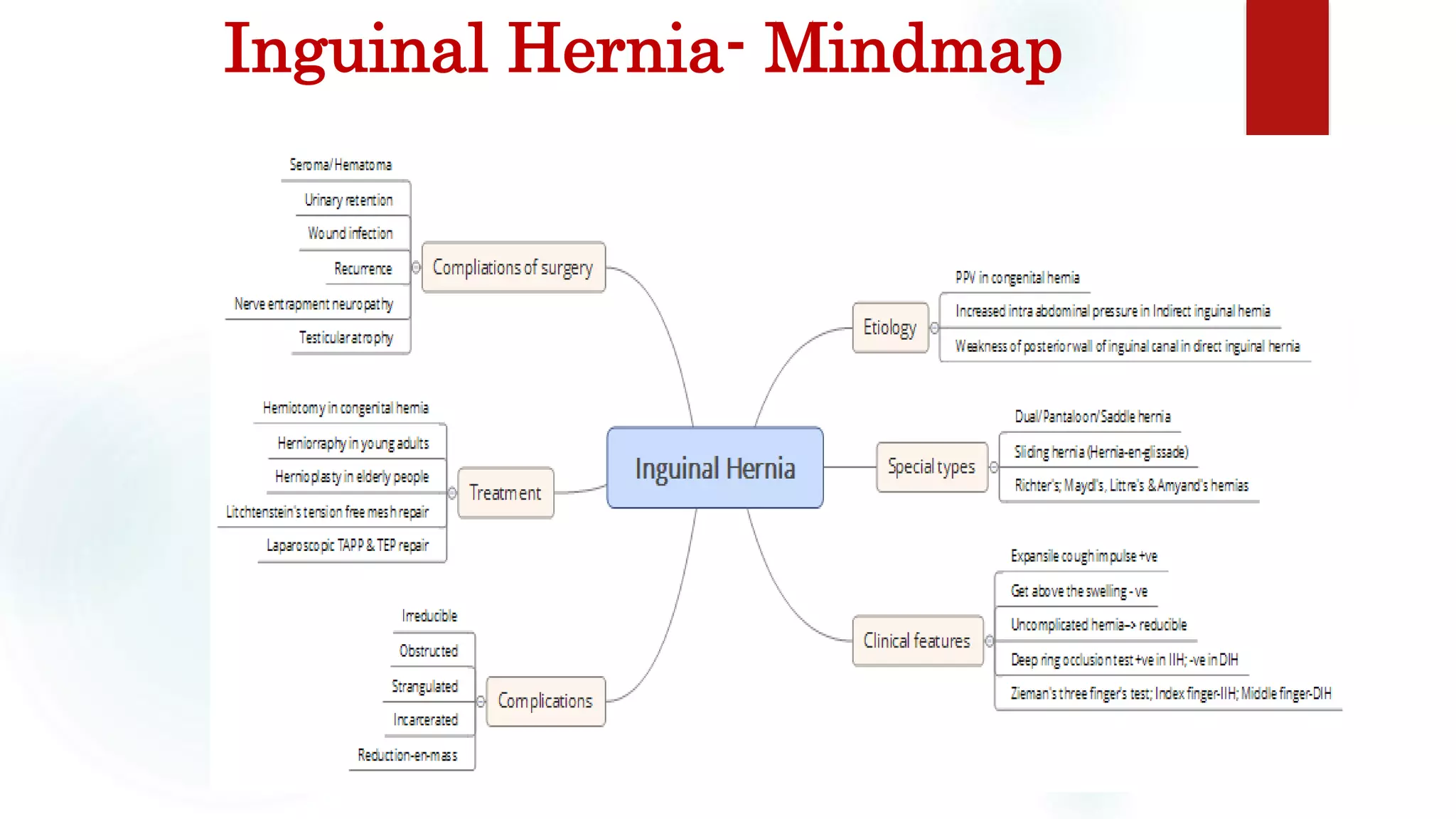




The document provides a detailed overview of inguinal hernia, including its causes, classifications, clinical features, and treatment options. It describes the clinical presentation of patients with groin swellings and differentiates between indirect and direct hernias, along with complications. Additionally, it outlines various surgical techniques and potential complications associated with hernia repairs.























































































