2. Introduction
• disorder characterized by a full-thickness intussusception of the
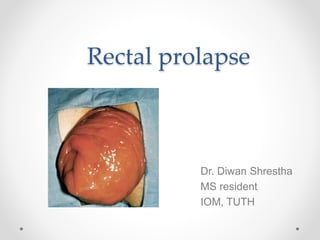
rectal wall, which protrudes externally through the anus
• Complete rectal prolapse
All layers of rectum prolapse
through the anal canal
• Partial or mucosal prolapse
Only the mucosal layer prolapse
• Internal prolapse
Rectum descends towards but does not pass through the anal canal
3. Anatomy of rectum
• 12 - 15 cm long
• Begins from rectosigmoid junction
• Ends at anorectal junction
• follows the curve of the sacrum in the true pelvis
• posterior surface is almost completely extraperitoneal
• possesses three curves known as the valves of Houston
• middle valve folds to the left
• proximal and distal valves fold to the right
4. Anatomy of rectum
• Upper 1/3rd – anterior & lateral surface
covered by peritoneum
• Middle 1/3rd - anterior peritoneal
covering only
• the lower 1/3 – no peritoneal covering
• Lower rectum separated from
other organs by fascial condensation
Anterior – fascia of Denonvillier
Posterior – fascia of Waldeyer
5. Anatomy of rectum
• Arterial supply
Superior rectal artery : branch of IMA
Middle rectal artery : branch of anterior
division of internal iliac
Inferior rectal artery : terminal branch of
internal pudendal artery
• Venous drainage
Corresponds to arteries
• Lymphatic drainage
Upper 2/3rd – paraaortic node
Lower 1/3rd – internal iliac node
6. Pelvic floor
• consists of the pubococcygeus, iliococcygeus, and puborectalis
• Pelvic diaphragm resides between the sacrum, obturator fascia,
ischial spines, and pubis
forms a strong floor that supports the pelvic organs
with the external anal sphincter, regulates defecation
• Puborectalis a strong, U-shaped sling of striated muscle course
around the rectum just above the level of the anal sphincters
Relaxation of the puborectalis straightens the anorectal angle and permits
descent of feces
contraction produces the opposite effect
7. Etiology
Two competing theories of rectal prolapse :
1. Alexis Moschcowitz in 1912
caused by a sliding herniation of the pouch of Douglas through the pelvic floor
fascia into the anterior aspect of the rectum
2. Broden & Snellman in 1968
a full-thickness rectal intussusception starting approx 3 inches above the
dentate line and extending beyond the anal verge
8. Etiology
• anatomic abnormalities
diastasis of the levator ani
abnormally deep cul-de-sac
a redundant sigmoid colon
a patulous anal sphincter
loss or attenuation of the rectal sacral attachments
• Chronic constipation with straining
• Multiparity
Nulliparity (35%)
• Pudendal nerve damage
Obstetric injury
Diabetes
9. Epidemiology
• Bimodal incidence
o One peak occurs in children within the first 3 years of life
o the second peak occurs after the seventh decade
• Rectal prolapse associated with children
o Equal in both sexes
o often associated with a diarrheal illness
o typically not a recurring problem and can be self-limited
• In the elderly
o rectal prolapse is more common in women (80% to 90%)
o prevalence increases with age
• Rectal prolapse may affect institutionalized patients
neurologic or psychiatric comorbidities (15%)
10. Clinical presentation
• Protuberance or bulge from the anus
• mucus discharge
• Rectal bleeding
• Fecal incontinence
• Feeling of incomplete evacuation
• Chronic constipation
• Rectal pain in early prolapse
less in patients with long-standing prolapse
Uncomfortable sensation of sitting on a mass within anal canal
• Urinary incontinence (35%)
11. Clinical presentation
• Some patients experience rectal incarceration or even strangulation
a large, painful, immobile rectal mass
• Patients with internal intussusception
obstructed defecation
severe abdominal pain
12. Rectal prolapse Hemorrhoid
Tissue folds Circumferential Radial
Sulcus between prolapse
& rectum
circumferential none
Abnormality on palpation Double rectal wall hemorrhoidal plexus
Resting & squeeze
pressure
decreased normal
Easily reducible &
painless
Extreme pain & can be
accompanied by fever
13. Evaluation
• On standing or Valsalva
Visualisation of prolapse
• DRE
Lax anal sphincter
Diminished squeeze efforts
• Proctosigmoidoscopy
Erythematous, edematous rectal mucosa
Solitary rectal ulcer in mid rectum
• Anal manometry
Normal resting and squeeze values are 40 to 80 mm Hg
14. Evaluation
• Pudendal nerve terminal motor latency test
Values between 1.8 and 2.2 milliseconds normal
• Dynamic MRI
Redundant, prolapsing rectosigmoid
• Triple contrast cinedefecography
Delineate complex floor abnormalities
• Defecography
Evaluates anatomic abnormalities, such as rectocele, enterocele, and vaginal
vault prolapse
15. Defecography grading system of
intussuseption
Grade Description
N Rectum remains fixed to sacrum, sphincter relaxes &
rectum empties
1 Nonrelaxation of puborectalis
2 Mild intussuseption or mobility from sacrum
3 Moderate intussuseption
4 Severe intussuseption
5 Prolapse
R Rectocele
16. Treatment
Acute condition ( non complicated )
• Reduction – immediate management
Continuous, steady pressure
Applying table salt or sugar to the mucosa reduce swelling of incarcerated
rectum
Elastic compression wrapping
Hyaluronidase injection into the prolapsed rectum
17. Treatment
In infants & young children
• Digital repositioning
Parents are taught to replace the protusion
Any underlying causes addressed
• Submucosal injections
If digital repositioning fails after 6 weeks trial, 5% phenol in almond oil injected
under GA
• Surgery
Child placed in prone jack knife position
Rectum sutured to sacrum
18. Surgical treatment
• More than 100 different surgical procedures
• Goal
Elimination of rectal prolapse
Restoration of continence
• Choice of procedure based on
Patient age
Comorbidities
Operative risk
Associated anatomic abnormalities
Prior rectal or colonic surgery
19. Surgical treatment
• Can be :
1. Transabdominal
2. Perineal
1. Transabdominal approach : open or laparoscopic
a. Ripstein procedure
b. Well‘s procedure
c. Resection +/- rectopexy
d. Suture / mesh rectopexy
20. Transabdominal approach
• Advantages :
Low recurrence rates
Resection rectopexy improve the bowel habit of patients having
preoperative constipation
• Disadvantage :
High morbidity
Evacuation difficulties may occur after suture or mesh rectopexy
• Reserved for younger patients who can tolerate GA
21. Ripstein procedure
• Mobilization of rectum on both sides and
posteriorly down to the levator ani muscle
plate
• 5-cm band of rectangular mesh placed
around its anterior aspect at the level of the
peritoneal reflection
• both sides of the mesh sutured to presacral
fascia
• Recurrence rate : 2.5% to 5%
• Complication :
Constipation
large bowel obstruction
erosion of the mesh through the bowel
ureteric injury or fibrosis
small bowel obstruction
rectovaginal fistula
22. Well‘s procedure
• Mobilisation of rectum
• Mesh kept in posterior aspect of rectal
fascia proper
• Fixed to presacral fascia
• Recurrence rate : 3 – 5%
• Advantage : low constipation rate
23. Resection rectopexy
• Frykman and Goldberg
procedure
sigmoid colon and rectum
mobilized to the level of the
levators
Resection of the redundant
sigmoid colon
Anastomosis is completed
Rectopexy sutures are placed
• Recurrence : 2-5%
• Complication :
obstruction
anastomotic leak
24. 2. Perineal approach can be :
a. Altmeier procedure
Perineal rectosigmoidectomy
b. Delorme procedure
Mucosal sleeve resection
c. Thiersch procedure
Anal encirclement
25. Perineal approach
• Advantages :
Can be done under regional anesthesia
Low morbidity
Shorter hospital stay
• Disadvantages :
High recurrence rate
26. Altmeier procedure
• Redundant rectum extenalised
• Full thickness circumferential
rectal incision 1-2 cm proximal
to dentate line
• Vascular supply ligated
• Redundant rectum & sigmoid
colon resected
• Coloanal anastomosis either
handsewn or stapled
28. Delorme procedure• Rectal prolapse delivered
through anus
• Circumferential incision 2 cm
above dentate line through
mucosa & submucosal layer
• Mucosal sleeve stripped from
muscularis & plication done
using longitudinal suture
• Resection of excess stripped
mucosa
• Mucosal coloanal anastomosis
Recurrence : 12-31%
29. Thiersch procedure
• 2 small incisions made lateral
to external anal sphincter
• Submucosal tunnel created
around anus
• Wire inserted & advanced
around anal canal & tightened
• Can be done under LA
• Recurrence > 30%
31. Laparoscopic mesh rectopexy
• A periumbilical port is put in
place, followed by two
additional ports in the lower
abdomen (one in each
quadrant)
32. Laparoscopic mesh rectopexy
• mobilization of the rectum
• the nonabsorbable mesh is
rolled up and inserted through
a port
• The mesh is tacked to the
sacrum with a laparoscopic
stapler, and the lateral edges
of wrapped mesh are secured
to the rectal wall with sutures
36. Recurrent prolapse
• Can occur after either perineal or abdominal procedure
Overall recurrence – 15%
Abdominal procedure – up to 10%
Perineal procedure – up to 20%
37. Recurrent prolapse
• 2 types
Mucosal prolapse
Full thickness prolapse
• Early recurrence
Occur within first year after surgery
likely the result of a specific technical failure
incomplete mobilization of the rectum
inadequate fixation of the rectum to the sacrum
incomplete resection of a redundant sigmoid
vigorous physical activity
38. Recurrent prolapse
• Late recurrence
recurs beyond 1 year of surgery
results from persistence of the underlying pathophysiology
disordered defecation
abnormal intestinal motility
straining
• Currently,no standardized strategy for recurrent rectal prolapse
39. Recurrent prolapse
• Some authorities advocate an abdominal procedure for the second
operation, regardless of the initial operation (1)
• Some studies suggest that unless the previous anastomosis can be
resected in the second procedure, repeat resectional procedures
should be avoided(2)
• Perineal rectosigmoidectomies are an exception to this broad rule:
they can be safely repeated as long as the recurrent prolapse
contains the previous anastomosis.
• Subtotal colectomy should be considered in patients with slow
transit constipation without sphincter weakness
1. Hool GA et al, Surgical treatment of recurrent complete rectal prolapse. Dis Colon Rectum 1997
2. Fengler SA,, et al. Management of recurrent rectal prolapse. Dis Colon Rectum 1997
40. Rectal prolapse with solitary rectal ulcer
syndrome (SRUS)
• 80% of patients with SRUS have an associated rectal prolapse
• SRUS, a clinical condition characterised by rectal bleeding, copious
mucus discharge, anorectal pain & difficult evacuation
• Typically affect young female with an average age of 25 years
• The cause of SRUS unclear, but speculation centers on chronic
ischemia
41. Rectal prolapse with solitary rectal ulcer
syndrome
• gross pathologic features of SRUS can range from a typical crater-
like ulcer with a fibrinous central depression to a polypoid lesion
always located on the anterior aspect of the rectum, 4 to 12 cm from the anal
verge
• The rectal ulcer is usually found on proctoscopy or flexible
sigmoidoscopy
• Defecography, radiologic procedure of choice
reveals the underlying disorder
42. Rectal prolapse with solitary rectal ulcer
syndrome
• Symptomatic SRUS associated with asymptomatic prolapse
a trial of nonoperative therapy including pelvic floor retraining , dietary management,
short-term use of topical antiinflammatory medications containing mesalamine
if such therapy fails, surgical intervention considered
• In cases of symptomatic prolapse associated with asymptomatic
SRUS
healing of the ulcer can be demonstrated in one third of patients undergoing operation
for the prolapse
Abdominal repairs resulted in a cure rate of 80% in patients with SRUS and full-
thickness rectal prolapse
• Rarely, symptoms of severe bleeding, pain, and spasm may require a
temporary diverting sigmoid colostomy
43. References
1. Sabiston textbook of surgery, 20th Edition
2. Shackelford's Surgery of the Alimentary Tract, 8th Edition
3. Fischer‘s Mastery of Surgery, 7th Edition
Editor's Notes
There is some controversy about the definition of the proximal and distal extent of the rectum. Some consider the rectosigmoid junction to be at the level of the sacral promontory; others consider it to be the point at which the taeniae converge. Anatomists consider the dentate line the distal extent of the rectum, whereas surgeons typically view this union of columnar and squamous epithelium as existing within the anal canal and consider the end of the rectum to be the proximal border of the anal sphincter complex
These valves are more properly called folds because they have no specific function as impediments to flow. They are lost after full surgical mobilization of the rectum, a maneuver that may provide approximately 5 cm of additional length to the rectum
- Denonvilliers' fascia, a dense membrane between the rectum and the seminal vesicles, is also called the rectogenital fascia; Walderyer's fascia is a dense connective tissue layer between the posterior part of the rectal proper fascia and the presacral fascia at the levels of S3 and S4.
e. Both explanations take into consideration the weakness of the pelvic floor in rectal prolapse cases, the concept of herniation, and the observation that there are abnormal anatomic features that characterize this condition
hemorrhoids are collections of submucosal, fibrovascular, arterio-venous sinusoids mostly seen in the left lateral, right anterolateral and right posterolateral region of anal canal. While rectal prolapse is the intussusception of whole circumference of the rectal wall through the anal canal which presents with circular folds of rectal mucosa.
- Resting pressure reflects the function of the internal sphincter, whereas squeeze pressure measures external sphincter (voluntary muscle) contributions
Pudendal nerve terminal motor latency times are measured with a special transducer attached to a glove-like apparatus designed to be worn on the finger and hand a glove-like apparatus designed to be worn on the finger and hand. A digital rectal examination is required, with application of the finger electrode to the right and left levator ani complex. . Prolonged values are seen in traumatic injuries of the vagina or anal canal (obstetric in cause), sacral nerve root damage, or chronic diseases such as diabete
Dynamic MRI - Dynamic imaging (imaging obtained at rest, during squeezing, straining, and defecation)
Cinedefecography - defecation cycle is recorded as a continuous series
Defecography - Barium paste is placed in the vagina and rectum after the patient ingests a watersoluble contrast agent to opacify the small bowel. As the patient evacuates the rectal barium paste
Mild to mod intussuseption usually treated conservatively
grade 4 intussuseption may require resection of redundant rectum or rectopexy
- For example, doing a perineal proctosigmoidectomy if the patient had a prior rectal resection places the remaining bowel at risk of being devascularized.
- Abdominal approach can be done by open laparotomy, laparoscopically or robotically
Evacuation difficulties may continue to plague patients after suture or mesh rectopexies that may be due to stenosis by the foreign material or angulation of the redundant rectosigmoid.