Downloaded 910 times
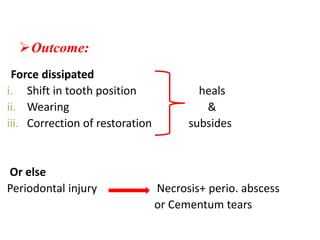
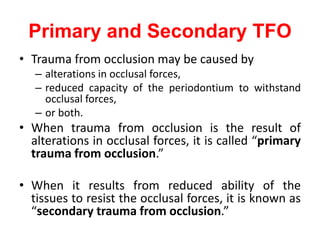
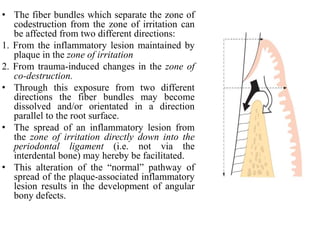

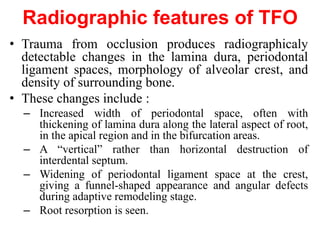


- Trauma from occlusion occurs when occlusal forces exceed the adaptive capacity of the periodontium, causing injury. It can be acute or chronic. - The magnitude, direction, duration, and frequency of forces impact the periodontium's ability to adapt. Excessive pressure or tension can damage tissues. - Primary trauma from occlusion is caused by changes in occlusal forces, while secondary trauma occurs when reduced bone support impairs the tissues' resistance to normal forces. - The periodontium responds to trauma in three stages - injury, repair through new tissue formation, and adaptive remodeling to better withstand forces. Trauma can cause reversible damage if forces are reduced, or lead to irreversible injury if






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















